
Abstract
The Centers for Disease Control and Prevention (CDC) asserts that “some HPV infections can be persistent and can progress to cancer in both women and men later in life.” When coupled with the CDC’s universality claim, this statement creates a misleading narrative of inevitable oncogenic progression. By presuming that the majority of the population is infected, the CDC implies that millions are at risk of cancer. Yet epidemiological data, clearance kinetics, and immune‑stratified analyses reveal that persistent infections represent less than 1% of the population at any given time, and progression to cancer is rarer still.
This article demonstrates that the CDC’s persistence narrative is pseudoscientific, unprovable, and disconnected from ground reality. Using the HPV Vaccines Biological Impossibilities (HVBI) Framework, we show that persistence is rare, progression is exceptional, and cancer incidence continues to decline independent of vaccination. The persistence claim, like the universality claim, collapses under scrutiny.
Introduction
The CDC’s persistence narrative is not an isolated statement but a continuation of its universality rhetoric. If 90% of the population were truly infected, then “some” persisting would imply millions of ongoing oncogenic cases. Yet SEER data confirm fewer than 15,000 cervical cancer cases annually in the United States, a figure incompatible with CDC’s infection backlog. More than 95% of HPV infections clear naturally within 1–2 years, even for high‑risk strains such as HPV‑16 and HPV‑18. The persistence narrative conflates transient viral DNA detection with rare oncogenic progression, exaggerating risk and justifying mass vaccination campaigns. This introduction situates the persistence claim within the broader pseudoscientific framework and sets the stage for systematic rebuttal.
Epidemiological Disproof Of Persistence
The CDC’s persistence narrative collapses when contextualized against clearance kinetics and cancer incidence data. More than 95% of HPV infections resolve spontaneously within two years, even for high‑risk strains. If persistence were proportional to CDC’s inflated infection figures, catastrophic cancer rates would be observed. Instead, SEER data confirm declining incidence from 13.1 per 100,000 women in the mid‑1970s to 7.7 in 2022, with mortality dropping to 2.2 per 100,000.
At any given time, fewer than 1% of the population harbors persistent infection, undermining the CDC’s implication of widespread oncogenic risk. The persistence narrative therefore exaggerates risk by conflating transient viral DNA detection with rare oncogenic progression.
Natural History And Clinical Timelines
The natural history of HPV infection demonstrates that persistence and progression are strongly modulated by immune competence. In individuals with normal immune systems, infections are overwhelmingly transient and clinically insignificant. Weak immune systems show persistence, but CIN2/3 typically appears only after a decade, with cancer risk emerging after 25–30 years. Fast progressors and immunocompromised individuals face much shorter timelines, with CIN2/3 appearing within 5–10 years and invasive cancer within 10–15 years. Treatment outcomes vary: slow progressors respond well, while fast progressors and immunocompromised patients face higher recurrence risks.
Table 1: Consolidated Natural History, Progression, And Clinical Timelines (HPV‑16/18, Base Year: 2010)
| Immune Category | Clearance / Persistence | CIN 2/3 Appearance | CIN 2/3 Duration | Invasive Cancer Timeline (No Treatment) | Time: Infection → AIS | Time: AIS → Cancer (No Treatment) | Screening at AIS Stage | Treatment at AIS Stage | Cancer Cases Despite Treatment (% of AIS) | Notes on Recurrence |
|---|---|---|---|---|---|---|---|---|---|---|
| Normal Immune System | >90% clear within 1–2 years | None | N/A | None | N/A | N/A | Not applicable | Not applicable | 0% | Infection transient, clinically insignificant |
| Weak Immune System (Slow Progressors) | Partial control; high persistence | 10–15 Years | 10–15 Years | 25–30 Years | ~25 Years → 2035 | ~5 Years → 2040 | Detectable at AIS (LEEP/cone usually curative) | High success; most cured | ~5–10% | Recurrence usually occurs after 2040 |
| Very Weak Immune System (Fast Progressors) | Poor control; rapid persistence | 5–10 Years | ~5 Years | 10–15 Years | ~15 Years → 2025 | ~5 Years → 2030 | Detectable at AIS (requires aggressive excision) | Moderate success; higher recurrence risk | ~15–20% | Recurrence can occur within or just beyond 2030 |
| Immune‑Compromised (HIV / Severe Suppression) | Accelerated persistence | 3–5 Years | <2 Years | 5–10 Years | ~7 Years → 2017 | ~3 Years → 2020 | Detectable at AIS (needs strict monitoring) | Lower success; hysterectomy often required | ~25–30% | Recurrence often rapid |
Analysis:
This table demonstrates that persistence is not a universal phenomenon but a rare outcome tied to immune weakness. In normal immune systems, infections are transient and clinically insignificant, with no progression to CIN2/3 or cancer. Weak immune systems show persistence only after a decade, and even then, progression to invasive cancer requires 25–30 years. Fast progressors and immunocompromised individuals face shorter timelines, but these represent small subgroups of the population. Treatment outcomes vary, but even in high‑risk groups, recurrence rates remain limited. The data confirm that persistence is rare, progression rarer still, and cancer incidence is far below the catastrophic levels implied by CDC’s narrative.
Stage‑Based Testing Strategy
The CDC’s conflation of transient viral DNA detection with inevitable cancer progression is scientifically indefensible. A stage‑based analysis reveals that CIN1 and CIN2 often regress, while only CIN3 represents a true pre‑cancerous condition requiring intervention. Indiscriminate molecular testing exaggerates risk and leads to overtreatment, while targeted testing optimizes benefit‑harm balance.
Table 2: Stage‑Based Testing Strategy (HPV‑16/18)
| Stage | Natural Course | Risk of Over‑Testing | Safe Testing / Intervention Window | Rationale |
|---|---|---|---|---|
| Initial Infection (HPV DNA+, no lesions) | ≈95% clear within 1–2 years | Very high – most infections resolve naturally | Retest only if infection persists beyond 18–24 months | Early testing causes anxiety and overtreatment |
| CIN1 (low‑grade changes) | 90% of persistent cases regress | High – regression is common | Repeat cytology/HPV testing in 12 months | Observation preferred |
| CIN2 (moderate changes) | Some regress, some progress | Moderate – depends on age and persistence | Monitor closely; treat if persistent | Balances regression potential with risk of progression |
| CIN3 (high‑grade changes) | Precancerous, unlikely to regress | Low – intervention justified | Immediate treatment (LEEP, conization) | True intervention point |
| AIS → Cancer | Rapid progression once AIS develops | N/A | Prevention relies on CIN3 detection | Detecting CIN3 early avoids progression |
Analysis:
This table highlights the danger of indiscriminate molecular testing. At the initial infection stage, ≈95% of cases clear naturally, meaning early testing leads to unnecessary anxiety and overtreatment. CIN1 and CIN2 often regress, making observation the preferred strategy. Only CIN3 represents a true intervention point, where treatment is justified and effective. AIS progresses rapidly to cancer, but prevention relies on detecting CIN3 early. The HVBI Framework demonstrates that targeted, stage‑based testing achieves superior benefit‑harm balance compared to universal molecular screening, dismantling the CDC’s persistence narrative.
Comparative Analysis Of CDC Persistence Claim vs HVBI Framework
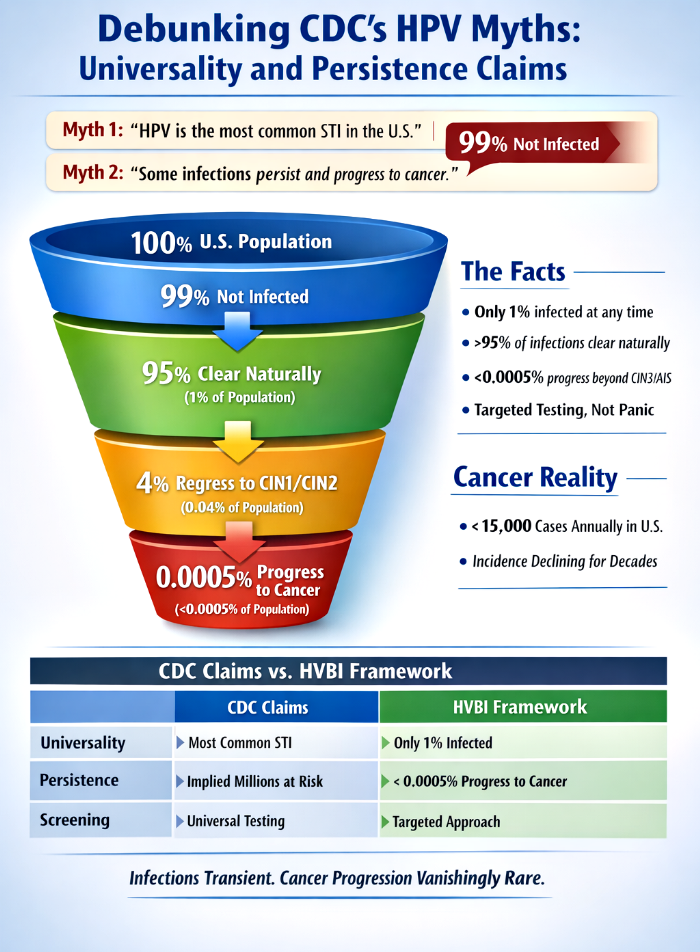
The persistence narrative can be directly contrasted with the HVBI Framework. While the CDC frames persistence as a significant threat, the HVBI Framework demonstrates that persistence is rare, progression rarer still, and cancer incidence continues to decline. Transparent statistics show that only 1% of the population is infected at a given time, 95% of these clear naturally, 4% regress at CIN1/CIN2, and only 1% of 5% of 1% progress beyond CIN3/AIS. This translates to less than 0.0005 of the total population — a vanishingly rare outcome.
Table 3: Comparative Analysis Of CDC Persistence Claim vs HVBI Framework
| Aspect | CDC Claim | HVBI Framework Evidence |
|---|---|---|
| Persistence | “Some infections persist and progress” | Transparent statistics show only 1% of the population is infected at a given time. Of this 1%, 95% clear naturally, 4% regress at CIN1/CIN2, and only 1% of 5% of 1% progress beyond CIN3/AIS. Persistence is therefore <0.0005 of the total population — vanishingly rare. |
| Cancer Risk | Implied millions at risk | Actual burden is fewer than 15,000 cervical cancer cases annually in the U.S.; incidence and mortality have been declining for decades, independent of vaccination. |
| Biological Basis | DNA detection conflated with pathology | Clearance kinetics show >95% of infections resolve naturally; persistence requires rare immune evasion and does not equate to cancer. |
| Screening Strategy | Universal molecular testing | Targeted immune‑stratified approach: PCR/genotyping reserved for persistent infections beyond clearance windows, older individuals with concerning cytology, and immunocompromised patients. |
Analysis Of Table 3
This comparative table exposes the fundamental weakness in the CDC’s persistence narrative. By stating that “some infections persist and progress,” the CDC implies a significant public health burden. Yet transparent statistics reveal that only 1% of the population is infected at any given time, and of this small fraction, 95% clear the infection naturally. The remaining 5% are not destined for cancer; 4% regress at CIN1 and CIN2 stages, leaving only 1% of 5% of 1% — less than 0.0005 of the total population — progressing beyond CIN3/AIS. This vanishingly small risk dismantles the CDC’s suggestion of widespread persistence and progression.
The cancer risk narrative is equally misleading. If persistence were as common as the CDC implies, millions of cancers would be expected annually. Instead, SEER data confirm fewer than 15,000 cervical cancer cases per year in the United States, with incidence and mortality declining steadily for decades, independent of vaccination. The biological basis of the CDC’s claim is flawed, as it conflates transient DNA detection with pathology. More than 95% of infections resolve naturally, and persistence requires rare immune evasion. Screening strategies further highlight the disconnect: universal molecular testing exaggerates risk and leads to overtreatment, while targeted immune‑stratified approaches achieve superior benefit‑harm balance. Together, these analyses confirm that the CDC’s persistence claim is pseudoscience, disconnected from biological and epidemiological reality.
Broader Implications Of The Persistence Narrative
The CDC’s persistence claim is not simply a scientific statement; it functions as a rhetorical device that exaggerates risk and justifies mass vaccination campaigns. By presenting persistence as a common outcome, the CDC implies that millions of individuals are at risk of cancer, despite epidemiological data showing otherwise. This narrative conflates transient viral DNA detection with pathology, ignoring the biological reality that more than 95% of infections resolve naturally. The transparent statistics demonstrate that persistence is vanishingly rare, occurring in less than 0.0005 of the total population. Such a small risk cannot justify the sweeping generalizations and fear‑based messaging embedded in the CDC’s persistence claim.
The persistence narrative also undermines rational public health policy. By exaggerating risk, it encourages indiscriminate molecular testing and mass vaccination strategies that yield minimal benefit and substantial harms and deaths. Over‑testing leads to anxiety, unnecessary procedures, and overtreatment, while mass vaccination campaigns are justified on the basis of inflated infection and persistence figures. In contrast, the HVBI Framework demonstrates that targeted, immune‑stratified screening strategies achieve superior benefit‑harm balance, focusing resources on high‑risk individuals while avoiding unnecessary interventions in the vast majority of the population.
Conclusion
First, the CDC’s claim that some HPV infections persist and progress to cancer is not an epidemiological fact but a rhetorical device designed to exaggerate risk and justify mass vaccination campaigns. Transparent statistics reveal that only 1% of the population is infected at a given time, 95% of these clear naturally, 4% regress at CIN1/CIN2, and only 1% of 5% of 1% progress beyond CIN3/AIS. Persistence is therefore vanishingly rare, occurring in less than 0.0005 of the total population.
Second, the CDC’s persistence narrative collapses when contextualized against clearance kinetics and cancer incidence data. If persistence were proportional to CDC’s inflated infection figures, catastrophic cancer rates would be observed. Instead, SEER data confirm fewer than 15,000 cervical cancer cases annually in the United States, with incidence and mortality declining steadily for decades, independent of vaccination.
Third, the CDC’s conflation of transient viral DNA detection with inevitable pathology is scientifically indefensible. Stage‑based testing reveals that only CIN3 represents the decisive intervention point, and inflated persistence figures risk fear‑based messaging and unnecessary interventions. The HVBI Framework provides a biologically grounded progression model that dismantles the CDC’s persistence narrative.
Finally, immune‑stratified screening strategies demonstrate the superiority of targeted PCR/genotyping over indiscriminate molecular testing. Routine early testing yields minimal benefit and substantial harms, while targeted testing optimizes benefit‑harm balance. Implementing immune‑informed PCR triage reduces unnecessary procedures, concentrates resources on high‑risk individuals, and supports patient‑centered, evidence‑based screening policies.
In light of these analyses, the CDC’s persistence claim is unscientific, pseudoscientific, and disconnected from ground reality—just as its universality claim was. Together, these narratives form a foundation of pseudoscience that must be dismantled to restore integrity to public health discourse and to promote rational, evidence‑based strategies that respect biological reality and epidemiological truth.