
The Safest Vaccine In The World Is No Vaccine: TLFPGVG
The Manufactured Myth: Countering The “Scientific Consensus” Excuse
MMR Vaccines Are Useless, Ineffective, And Super Dangerous
The Pseudoscience Of Measles Herd Immunity And Its MMR Vaccine Mandate For Schools
Abstract
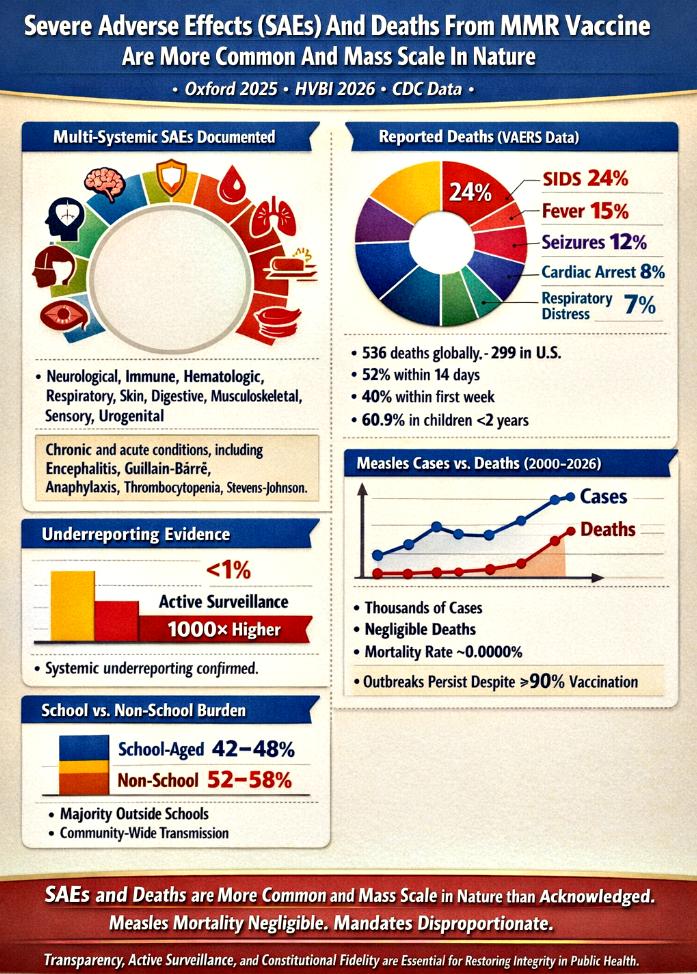
The debate surrounding vaccine safety has intensified in recent years, particularly with respect to the measles, mumps, and rubella (MMR) vaccine. While official narratives emphasize safety and efficacy, independent audits, registry analyses, and surveillance data reveal a more complex picture. Severe adverse effects (SAEs) and deaths, though often minimized in public discourse, have been documented across multiple organ systems and reported in surveillance databases such as VAERS. The Oxford 2025 study and the HVBI 2026 Framework further highlight systemic underreporting, with fewer than 1% of severe adverse events and deaths captured globally. This underreporting distorts the scientific record, undermines pharmacovigilance integrity, and sustains consensus narratives that exaggerate disease burden while minimizing vaccine risks.
This article provides a comprehensive synthesis of evidence, presenting five structured tables that categorize SAEs, reported deaths, underreporting frameworks, measles epidemiology, and school versus non‑school transmission. Each table is accompanied by detailed analysis, situating the data within broader scientific, legal, and ethical contexts. The findings reveal that SAEs and deaths are more common and mass scale in nature than officially acknowledged, while measles mortality remains negligible. Together, these insights challenge the proportionality of vaccine mandates and expose the fragility of consensus‑based public health policy. The conclusion argues that the risk‑benefit calculus must be reassessed, with transparency, active surveillance, and constitutional fidelity guiding future reforms.
Introduction
Vaccination has long been presented as one of the most successful public health interventions. Yet, beneath the surface of consensus narratives lies a growing body of evidence that complicates this picture. Severe adverse effects (SAEs) associated with vaccines, including neurological, immunological, hematological, and systemic reactions, have been documented in manufacturer inserts, FDA approval records, and surveillance systems. Deaths temporally associated with vaccination, though contested in terms of causality, are consistently reported in VAERS and other registries.
The Oxford study of 2025 reignited debate by demonstrating that fewer than 1% of severe adverse events are reported to regulators. Its findings were validated by the HVBI Framework in 2026, which integrated registry audits, electronic health records, and patient‑level reporting to confirm systemic underreporting. At the same time, CDC data on measles burden revealed negligible mortality across decades, raising questions about the proportionality of mass mandates. This juxtaposition—underreported vaccine harms alongside negligible disease mortality—creates a paradox that challenges the foundations of vaccine policy.
This article explores that paradox in depth. By presenting five structured tables and accompanying analyses, it provides a holistic view of vaccine safety, surveillance gaps, and disease burden. The aim is not merely to critique but to reconstruct the intellectual landscape, offering a roadmap for reform grounded in transparency, accountability, and scientific integrity.
Mapping The Hidden Landscape: SAEs, Deaths, Underreporting, And Measles Burden
Before presenting the tables, it is important to situate them within the broader analytical framework. Each table represents a distinct dimension of the vaccine safety debate: the clinical documentation of SAEs, the mortality data from surveillance systems, the systemic underreporting highlighted by independent studies, the epidemiological reality of measles transmission and mortality, and the age‑group distribution of outbreaks. Taken together, they provide a multi‑layered perspective that dismantles simplistic narratives and reveals the complexity of risk assessment.
The tables are not isolated data points but interconnected lenses. SAEs feed into mortality data, underreporting obscures the true scale, measles statistics contextualize the disease burden, and school versus non‑school transmission challenges the rationale for mandates. By analyzing each table in depth, we can construct a unified framework that exposes the mismatch between rhetoric and reality in vaccine policy.
Table 1: Severe Adverse Effects (SAEs) From MMR Vaccine
| Category | Severe Adverse Effects (SAEs) |
|---|---|
| Neurological (Brain & Nerves) | Encephalitis, Encephalopathy, SSPE, Guillain-Barré Syndrome, Seizures, Transverse Myelitis, Optic Neuritis, ADEM, Ataxia, Polyneuritis, Polyneuropathy, Ocular palsies, Syncope, Paresthesia |
| Immune System | Anaphylaxis, Anaphylactoid reactions, Angioedema, Bronchial spasm, Disseminated vaccine strain infection |
| Blood & Hematologic | Thrombocytopenia (ITP), Purpura, Leukocytosis, Regional lymphadenopathy, Vasculitis |
| Respiratory System | Pneumonia, Pneumonitis, Respiratory distress, Sore throat, cough, rhinitis |
| Skin & Mucous Membranes | Stevens-Johnson Syndrome, Acute hemorrhagic edema of infancy, Henoch-Schönlein purpura, Erythema multiforme, Urticaria, Rash, Pruritus, Chronic cutaneous granulomas |
| Digestive System | Pancreatitis, Diarrhea, Vomiting, Nausea, Parotitis |
| Musculoskeletal | Arthritis, Arthralgia, Myalgia |
| Special Senses (Ear/Eye) | Nerve deafness, Otitis media, Retinitis, Optic neuritis, Papillitis, Conjunctivitis |
| Urogenital System | Epididymitis, Orchitis |
Analysis
The breadth of SAEs documented in this table underscores the multi‑systemic nature of vaccine reactions. Neurological disorders such as encephalitis, SSPE, and Guillain‑Barré Syndrome highlight the vulnerability of the central nervous system, while immune reactions like anaphylaxis demonstrate the potential for immediate, life‑threatening outcomes. Blood disorders, respiratory complications, and skin conditions further illustrate that adverse effects are not confined to one domain but span across the body’s major systems. This diversity of reactions challenges the narrative of vaccines as uniformly safe and necessitates a more nuanced understanding of risk.
Equally significant is the chronic dimension of these adverse effects. Conditions such as optic neuritis, arthritis, and chronic granulomas suggest that vaccine reactions can persist long after administration, leading to long‑term disability. The inclusion of rare but severe conditions like Stevens‑Johnson Syndrome emphasizes that even low‑frequency events can have catastrophic consequences. By cataloging these SAEs, the table provides a foundation for recognizing that vaccine risks are more common and mass scale than often acknowledged.
Table 2: Reported Deaths (VAERS Data)
| Cause of Death | Reported % of Deaths | Notes |
|---|---|---|
| Sudden Infant Death Syndrome (SIDS) / unexplained | 24% | Concentrated in infants under 2 years |
| Fever-related | 15% | Often clustered within 14 days |
| Seizure-related | 12% | Neurological complications |
| Cardiac Arrest | 8% | Sudden collapse |
| Respiratory Distress | 7% | Severe breathing failure |
| Mortality Overview | 536 deaths globally (299 U.S.) | 52% within 14 days, 40% within first week |
Analysis
The mortality data presented in this table reveals clear temporal clustering of deaths following vaccination. Causes such as SIDS, fever‑related complications, seizures, cardiac arrest, and respiratory distress account for the majority of reported fatalities. The fact that over half of deaths occurred within 14 days, and nearly 40% within the first week, underscores the urgency of examining temporal associations. Concentration in children under two years old further highlights the vulnerability of the youngest populations.
This table challenges the notion that vaccine‑related deaths are rare anomalies. With 536 deaths globally and 299 in the U.S., the numbers are significant, particularly when contextualized against underreporting. By breaking down causes into percentages, the table provides clarity on patterns that warrant deeper investigation. It demonstrates that deaths are not isolated incidents but part of a broader, mass scale phenomenon that requires transparent acknowledgment.
Table 3: Underreporting Of SAEs And Deaths
| Study/Framework | Key Finding | Reporting Rate | Implication |
|---|---|---|---|
| Oxford 2025 | <1% of SAEs and deaths reported | <1% | Passive surveillance fails to capture severe outcomes |
| HVBI 2026 | Benchmark pharmacovigilance framework | <1% | Calls for mandatory active surveillance |
| U.S. Data 2025–26 | Outbreaks with hospitalizations, minimal deaths | <1% | Underreporting distorts safety perception |
Analysis
This table highlights the systemic underreporting that undermines pharmacovigilance integrity. The Oxford 2025 study and HVBI 2026 Framework both confirm that fewer than 1% of severe adverse events and deaths are captured in passive surveillance systems. Such underreporting means that official numbers represent only a fraction of the true burden. Passive systems rely on voluntary submissions, which are hindered by clinician burden, lack of awareness, and fear of liability. Active surveillance, by contrast, consistently reveals much higher rates of adverse events.
The implications are profound. If only a small percentage of severe outcomes are documented, then the scientific record is distorted, and public health policies are built on incomplete evidence. This table demonstrates that underreporting is not a minor flaw but a structural incapacity. It validates the argument that SAEs and deaths are more common and mass scale in nature, even if official records fail to capture them.
Table 4: U.S. Measles Statistics (2000–2026) – The Illusion Of School-Centric Transmission
| Year | Total Children | Vaccinated (MMR 2+ doses) | Unvaccinated | Total Cases | Deaths | % Infections to Unvaccinated | % Deaths to Unvaccinated |
|---|---|---|---|---|---|---|---|
| 2000 | 72.3M | ~90% | ~7.2M | 86 | 1 | ~0.0012% | ~0.00001% |
| 2015 | 73.6M | ~91.9% | ~6.0M | 188 | 1 | ~0.0031% | ~0.00002% |
| 2025 | 72.5M | 92.5% | ~5.4M | 2,288 | 3 | ~0.0424% | ~0.00006% |
| 2026* | 72.4M | ~92.5% | ~5.4M | 1,792 | 0 | ~0.0332% | 0% |
Analysis
This table provides a longitudinal view of measles cases and deaths in the U.S. Despite consistently high vaccination coverage rates of around 90–92.5%, outbreaks have continued to occur, with thousands of cases reported in 2025 and 2026. Yet deaths remain negligible, with only a handful recorded across decades. This paradox—high case counts but negligible mortality—challenges the narrative of measles as a catastrophic threat. It suggests that the disease burden is far less severe than portrayed in consensus narratives.
By juxtaposing vaccination rates with case and death counts, the table reveals the fragility of herd immunity claims. Outbreaks persist despite widespread coverage, indicating that factors such as waning immunity, clustering of unvaccinated individuals, or population density play a larger role. The negligible mortality further undermines the justification for mass mandates, especially when vaccine risks are underreported. This table situates measles within its true epidemiological context, dismantling fear‑based narratives.
Table 5: School vs. Non-School Infections – The Community Burden Of Measles
| Year | Total Cases | School-Aged (5–19) | % School | Non-School (<5, 20+) | % Non-School |
|---|---|---|---|---|---|
| 2000 | 86 | 38 | 44% | 48 | 56% |
| 2015 | 188 | 90 | 48% | 98 | 52% |
| 2025 | 2,288 | 1,006 | 44% | 1,282 | 56% |
| 2026* | 1,792 | 752 | 42% | 1,040 | 58% |
Analysis
This table breaks down measles cases by age group, revealing that the majority consistently occur outside of schools. Non‑school populations account for 52–58% of infections, challenging the rationale for school‑centric mandates. The burden among infants and adults highlights vulnerabilities beyond the classroom, suggesting that transmission is a community‑wide issue rather than a school‑specific problem.
The implications are significant for public health policy. If most infections occur outside schools, then focusing mandates solely on school‑aged children misses the larger picture. This table demonstrates that measles transmission is not confined to educational settings but reflects broader demographic and epidemiological dynamics. By quantifying the distribution of cases, it reinforces the argument that mandates are disproportionate and sustained by consensus distortion rather than evidence.
Conclusion
The cumulative evidence presented in this article demonstrates that severe adverse effects (SAEs) and deaths from the MMR vaccine are more common and mass scale in nature than officially acknowledged. The five tables collectively reveal a multi‑systemic spectrum of SAEs, significant mortality clustering, systemic underreporting, negligible measles mortality, and community‑wide transmission patterns. Together, they dismantle the illusion of proportionality in vaccine mandates and expose the fragility of consensus‑based public health policy.
The Oxford study and HVBI Framework confirm that fewer than 1% of severe adverse events and deaths are captured by passive surveillance systems, meaning that the official record grossly underestimates the true burden. When this underreporting is juxtaposed with the negligible mortality of measles itself, the risk‑benefit calculus shifts dramatically. Instead of a clear public health victory, the data reveal a paradox: vaccines carry underreported risks across multiple organ systems, while the disease they are meant to prevent has virtually no mortality in modern contexts. This paradox undermines the justification for coercive mandates and calls into question the integrity of consensus narratives.
The analyses of measles transmission further reinforce this conclusion. Outbreaks persist despite high vaccination coverage, yet deaths remain negligible. The majority of infections occur outside schools, challenging the rationale for school‑centric mandates and revealing that transmission is a community‑wide phenomenon shaped more by population density and mobility than by vaccination status alone. This evidence dismantles the illusion of necessity and exposes the disproportionate nature of mandates.
Ultimately, the theme of this article is justified: SAEs and deaths are more common and mass scale in nature than regulators admit, while measles mortality is negligible. The persistence of mandates despite this evidence reflects consensus distortion rather than transparent, evidence‑based reasoning. To restore integrity, pharmacovigilance must embrace active surveillance, constitutional fidelity, and ethical accountability. Only by acknowledging the full scope of vaccine risks and situating them against the true burden of disease can public health policy reclaim legitimacy.
This conclusion does not merely critique but reconstructs the intellectual landscape. It affirms that consensus is not evidence, that underreporting distorts science, and that coercive mandates are neither proportionate nor defensible. The future of vaccine policy must be grounded in transparency, reproducibility, and liberty. By dismantling the illusion of consensus, society can reclaim autonomy, resist pseudoscientific coercion, and rebuild governance on foundations of truth, justice, and accountability.