
The Safest Vaccine In The World Is No Vaccine: TLFPGVG
The VBHI Pseudoscience Framework Warns Against MMR Vaccines: A Forensic And Legal Analysis
Abstract
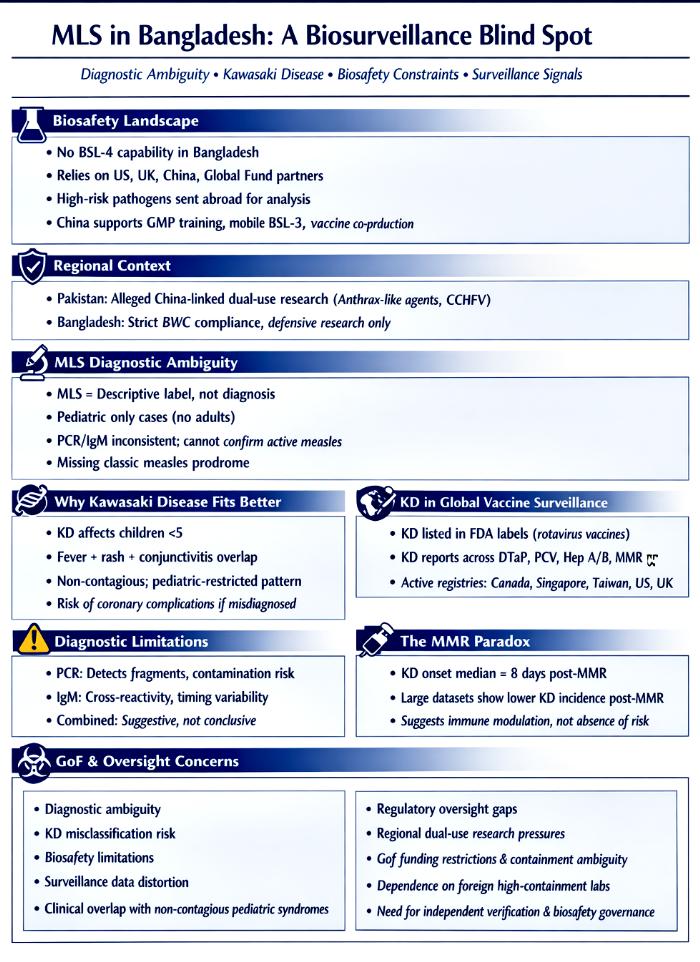
Bangladesh’s recent reports of “measles‑like symptoms” (MLS) among children have raised complex questions about diagnostic certainty, biosurveillance capacity, and the geopolitical context of high‑containment laboratory infrastructure. While official narratives attribute the outbreak to measles, the epidemiological pattern—pediatric‑only fatalities, absence of adult cases, and inconsistent laboratory confirmation—suggests a more nuanced reality. This article applies the VBHI Pseudoscience Framework to examine MLS as a diagnostic construct shaped by uncertainty, institutional limitations, and global partnerships. Bangladesh possesses multiple BSL‑3 laboratories but lacks BSL‑4 capability, relies heavily on international partners for high‑risk pathogen analysis, and operates within a regional environment where neighboring Pakistan has been accused of engaging in dual‑use research with China. These structural constraints shape how outbreaks are interpreted, investigated, and communicated.
The analysis is also examining the clinical overlap between measles and Kawasaki disease (KD), the limitations of PCR and IgM assays, and the documented presence of KD in global vaccine surveillance systems. KD appears in FDA labels, active surveillance registries, and post‑marketing safety networks across multiple countries, complicating the interpretation of MLS during immunization campaigns. The article also explores concerns surrounding gain‑of‑function (GoF) research in Bangladesh, where high‑fatality pathogens such as Nipah virus and H5N1 are studied in facilities that have historically faced biosafety and oversight challenges.
By integrating biosafety infrastructure, diagnostic uncertainty, vaccine surveillance data, and regional geopolitical dynamics, this article argues that MLS in Bangladesh cannot be understood solely as a measles outbreak. Instead, it reflects a convergence of structural vulnerabilities, clinical ambiguity, and global biosecurity pressures. Transparent investigation, strengthened biosafety governance, and independent diagnostic verification are essential to restoring public trust and ensuring accurate outbreak interpretation.
Introduction
Bangladesh occupies a unique position in the global biosurveillance landscape. As a densely populated country with endemic high‑risk pathogens such as Nipah virus and avian influenza H5N1, it faces recurring public‑health challenges that demand robust diagnostic and containment capabilities. Yet Bangladesh’s biosafety infrastructure remains uneven: while the country operates several BSL‑3 laboratories, it lacks any operational BSL‑4 facility. Extreme‑risk pathogens must be shipped abroad for analysis, creating structural dependencies that shape outbreak narratives and diagnostic certainty.
Against this backdrop, the emergence of “measles‑like symptoms” (MLS) among children has generated widespread concern. Official reports attribute the outbreak to measles, but the epidemiological pattern is atypical. Measles is a highly contagious virus that affects both children and susceptible adults; yet MLS cases in Bangladesh have been confined almost exclusively to children, with no corresponding adult infections. Laboratory confirmation has been inconsistent, relying heavily on PCR and IgM assays that detect fragments or immune responses rather than active infection. These limitations create diagnostic ambiguity that can obscure alternative explanations.
Kawasaki disease (KD), a pediatric vasculitis with overlapping clinical features, emerges as a plausible differential diagnosis. KD is documented in vaccine surveillance systems across multiple countries and appears in FDA labels for rotavirus vaccines. Active surveillance registries in Canada, Singapore, Taiwan, the United States, and the United Kingdom have identified KD clusters within 0–42 days of vaccination. The persistence of KD in regulatory and surveillance data complicates the interpretation of MLS during immunization campaigns.
This article provides the structural foundation for understanding why MLS has become a contested diagnostic category. Bangladesh’s reliance on international partners for high‑containment diagnostics, its expanding but uneven biosafety infrastructure, and its proximity to regional dual‑use research allegations create an environment where diagnostic uncertainty can be amplified. This article integrates these structural factors with clinical, epidemiological, and surveillance data to provide a comprehensive analysis of MLS in Bangladesh.
Section 1: Biosafety Infrastructure And Structural Vulnerabilities
Bangladesh’s high‑containment laboratory landscape is defined by a network of BSL‑3 facilities supported through extensive international collaboration. Institutions such as icddr,b, the Sylhet DR‑TB laboratory, and the MORU field labs operate with technical and financial support from partners including the US CDC, USAID, the University of Oxford, and The Global Fund. These partnerships have strengthened Bangladesh’s diagnostic capacity but also created dependencies that shape how outbreaks are investigated and interpreted. Without an operational BSL‑4 facility, Bangladesh cannot independently analyze the most dangerous pathogens, relying instead on foreign laboratories for confirmation. This structural limitation introduces delays, external influence, and potential blind spots in outbreak assessment.
China’s growing role in Bangladesh’s biosafety development is clear. Chinese partners provide training in Good Manufacturing Practices (GMP), high‑biosafety‑risk workshop management, and mobile BSL‑3 laboratory technology. These collaborations enhance Bangladesh’s capacity but also deepen its reliance on external expertise. Meanwhile, regional comparisons reveal stark asymmetries: Pakistan, Bangladesh’s neighbor, has been accused of engaging in dual‑use research with China, including work on high‑risk pathogens in BSL‑4‑equivalent facilities. While Bangladesh claims to maintain strict compliance with the Biological Weapons Convention (BWC), the regional environment underscores the importance of robust biosafety governance and independent diagnostic verification.
Section 2: Diagnostic Ambiguity And The MLS Construct
The term “measles‑like symptoms” is inherently ambiguous. It describes a constellation of fever, rash, and conjunctivitis that can arise from multiple conditions, including measles, rubella, roseola, scarlet fever, drug reactions, and Kawasaki disease. By treating MLS as synonymous with measles, public‑health authorities risk conflating distinct clinical entities under a single narrative. PCR and IgM assays, the primary tools used to support the measles hypothesis, have well‑documented limitations. PCR detects genetic fragments that may persist long after infection or arise from contamination, while IgM assays are prone to cross‑reactivity and timing variability. These limitations make it difficult to conclusively diagnose measles without clinical correlation and epidemiological consistency.
The epidemiological pattern of MLS in Bangladesh further complicates the measles narrative. Measles outbreaks typically affect both children and susceptible adults, yet MLS cases have been confined to children. This pediatric‑only pattern aligns more closely with Kawasaki disease, a non‑infectious vasculitis that primarily affects children under five. KD presents with fever, rash, conjunctivitis, mucous‑membrane changes, and extremity involvement—features that overlap with MLS. Misdiagnosis is plausible, especially in settings where diagnostic tools are limited and clinical expertise varies.
Section 3: Comparative Clinical Analysis
To understand the diagnostic ambiguity surrounding MLS, it is essential to compare the clinical and epidemiological features of measles and Kawasaki disease. Both conditions present with fever and rash, but their underlying mechanisms, age distributions, and complications differ significantly. The table below outlines these distinctions, providing a framework for interpreting MLS in Bangladesh.
Table 1: When Symptoms Deceive: Clinical And Epidemiological Contrasts Between Measles And Kawasaki Disease
| Feature | Measles | Kawasaki Disease |
|---|---|---|
| Age Distribution | Children & adults (if unvaccinated) | Primarily children <5 years |
| Prodrome | Fever, cough, coryza, conjunctivitis, Koplik spots | Prolonged fever ≥5 days, mucous‑membrane changes, extremity involvement |
| Rash | Descending maculopapular rash | Polymorphous rash, extremity peeling |
| Infectiousness | Highly contagious | Non‑contagious |
| Complications | Pneumonia, encephalitis | Coronary artery aneurysms, myocarditis |
| Diagnosis | PCR/IgM serology | Clinical criteria, inflammatory markers, echocardiography |
Analysis
The clinical distinctions between measles and Kawasaki disease reveal why MLS cannot be assumed to represent measles without rigorous diagnostic confirmation. Measles is characterized by a classic prodrome of cough, coryza, conjunctivitis, and Koplik spots, followed by a descending maculopapular rash. It is highly contagious and typically affects both children and susceptible adults. In contrast, Kawasaki disease presents with prolonged fever, mucous‑membrane changes, extremity involvement, and a polymorphous rash. It is non‑contagious and primarily affects children under five. The absence of adult cases in Bangladesh’s MLS outbreak is inconsistent with measles but aligns with KD’s age distribution. This epidemiological pattern suggests that KD should be considered a plausible differential diagnosis.
The complications associated with each condition further underscore the importance of accurate diagnosis. Measles can lead to pneumonia and encephalitis, while KD can cause coronary artery aneurysms and myocarditis. Misdiagnosing KD as measles could delay appropriate treatment, increasing the risk of long‑term cardiac complications. The reliance on PCR and IgM assays to support the measles hypothesis is problematic, given their limitations. PCR detects genetic fragments that may not indicate active infection, while IgM assays are prone to cross‑reactivity. Without clinical correlation and epidemiological consistency, these tests cannot conclusively diagnose measles. The MLS construct, therefore, reflects diagnostic ambiguity that must be addressed through comprehensive clinical evaluation and independent verification.
Section 4: Diagnostic Tools Under Scrutiny
Laboratory confirmation is often treated as the gold standard for diagnosing infectious diseases, but PCR and IgM assays have inherent limitations that can lead to misinterpretation. The table below outlines the intended purpose and limitations of these tests, highlighting why they cannot conclusively diagnose measles without clinical and epidemiological context.
Table 2: The Illusion Of Certainty: Limitations Of PCR And IgM In Measles Diagnosis
| Test | Intended Purpose | Limitations |
|---|---|---|
| PCR | Detect viral genetic material | Amplifies fragments, not live virus; contamination risk; false positives |
| IgM | Detect early immune response | Cross‑reactivity; variable timing; false positives/negatives |
| Combined Use | Suggestive evidence | Cannot prove active, transmissible infection |
Analysis
PCR’s sensitivity is both its strength and its weakness. While it can detect minute quantities of viral genetic material, it cannot distinguish between live virus and residual fragments. This limitation is particularly relevant in the context of MLS, where PCR positives may reflect contamination, past infection, or non‑specific amplification. The risk of false positives is heightened in high‑throughput settings where multiple samples are processed simultaneously. Without clinical correlation, PCR results can create a false sense of certainty that obscures alternative diagnoses such as Kawasaki disease.
IgM assays add another layer of complexity. IgM antibodies can cross‑react with unrelated pathogens, leading to false positives. The timing of IgM production varies among individuals, making it difficult to interpret results without considering the clinical timeline. When PCR and IgM are used together, they provide suggestive evidence but cannot conclusively diagnose active measles infection. The reliance on these tests to support the measles hypothesis in Bangladesh reflects a broader issue: the tendency to equate detection with proof. This conflation can lead to diagnostic errors, misclassification, and inappropriate public‑health responses.
Section 5: Vaccine Surveillance And The KD Connection
Kawasaki disease appears in vaccine surveillance systems across multiple countries, complicating the interpretation of MLS during immunization campaigns. The table below summarizes KD associations with various vaccines, drawing on regulatory documents and active surveillance registries.
Table 3: Signals In The System: Kawasaki Disease In Global Vaccine Surveillance Networks
| Vaccine Category | Specific Vaccines | Nature of Association |
|---|---|---|
| Rotavirus | RotaTeq, Rotarix, LLR | KD listed in FDA labels due to trial imbalances |
| Pneumococcal | PCV13, Pneumo 23 | Case reports in surveillance systems |
| Hepatitis | Hepatitis A/B | Individual case reports |
| Combination | DTaP‑IPV‑HepB‑Hib | KD reports in VAERS |
| Others | Influenza, MMR, BCG | Temporal KD occurrences |
Analysis
The presence of Kawasaki disease in vaccine surveillance systems is well‑documented. FDA labels for rotavirus vaccines list KD due to imbalances observed in clinical trials, while passive surveillance systems such as VAERS contain KD reports across multiple vaccine categories. These signals highlight the need for careful interpretation of MLS during immunization campaigns. KD’s appearance in regulatory documents and surveillance networks underscores its relevance as a differential diagnosis, particularly in settings where diagnostic tools are limited and clinical expertise varies.
Active surveillance registries provide further evidence of KD clustering within 0–42 days of vaccination. Programs in Canada, Singapore, Taiwan, the United States, and the United Kingdom have identified KD cases temporally associated with vaccines such as DTaP, PCV, and rotavirus. These findings are not speculative; they are documented in peer‑reviewed studies and regulatory reports. The overlap between KD incidence and routine immunization schedules complicates the interpretation of MLS in Bangladesh, where cases have been reported primarily among young children. Misdiagnosis is plausible, especially during mass vaccination campaigns.
Section 6: The MMR Paradox And Immune Modulation
The measles vaccine occupies a central position in the MLS narrative, yet surveillance data reveal a paradox: KD clusters occur within days of MMR vaccination. The table below summarizes key findings from global surveillance systems.
Table 4: The Measles Paradox: Kawasaki Disease Patterns In MMR Surveillance Data
| Surveillance Aspect | Findings |
|---|---|
| Temporal Onset | Median KD onset 8 days post‑MMR |
| Observed Risk | KD clusters suggest a direct association |
| Comparison | Fewer KD reports than DTaP or PCV |
| Diagnostic Certainty | 81% complete KD, 14% incomplete KD |
Analysis
The MMR–KD paradox highlights the complexity of interpreting surveillance data. KD clusters have been documented within days of MMR vaccination, suggesting a temporal association. The presence of KD clusters in surveillance systems cannot be ignored.
In the context of MLS in Bangladesh, the MMR paradox underscores the need for nuanced interpretation. If MLS cases coincide with measles vaccination campaigns, they represent misdiagnosed KD. The pediatric‑only pattern of MLS aligns with KD’s age distribution, while the absence of adult cases is inconsistent with measles. The reliance on PCR and IgM assays to support the measles hypothesis is problematic, given their limitations. A comprehensive approach that considers clinical, epidemiological, and surveillance data is essential to accurately interpret MLS.
Section 7: Biosafety, Gain‑Of‑Function, And Regional Dynamics
Bangladesh’s biosafety landscape is shaped by its status as a hotspot for high‑fatality pathogens such as Nipah virus and avian influenza H5N1. Research on these pathogens involves studying viral evolution, transmissibility, and antigenic drift—activities that can intersect with gain‑of‑function (GoF) concerns. Biosafety and oversight gaps are there in Bangladesh, including the use of BSL‑1/2 facilities for high‑risk testing and the ambiguous “BSL‑2+” designation. These gaps raise questions about containment, transparency, and regulatory oversight.
Regional dynamics further complicate the picture. Pakistan has faced allegations of engaging in dual‑use research with China, including work on high‑risk pathogens in BSL‑4‑equivalent facilities. While Bangladesh claims to maintain strict compliance with the Biological Weapons Convention (BWC), the regional environment underscores the importance of robust biosafety governance. The combination of high‑risk pathogens, containment mismatches, and shifting funding sources creates structural vulnerabilities that can influence outbreak interpretation. MLS must be understood within this broader context of biosafety capacity, geopolitical dynamics, and global biosecurity pressures.
Conclusion
The emergence of “measles‑like symptoms” in Bangladesh cannot be understood solely through the lens of infectious disease. This article reveals a biosafety landscape defined by structural vulnerabilities, international dependencies, and regional geopolitical dynamics. Bangladesh’s lack of BSL‑4 capability, reliance on foreign partners for high‑risk pathogen analysis, and uneven biosafety infrastructure create an environment where diagnostic ambiguity can be amplified. Supporting materials demonstrate that MLS overlaps clinically with Kawasaki disease, a pediatric vasculitis documented in global vaccine surveillance systems. The limitations of PCR and IgM assays further complicate the measles hypothesis, while the pediatric‑only pattern of MLS aligns more closely with KD.
The MMR paradox, vaccine surveillance data, and active registry findings underscore the need for nuanced interpretation of MLS during immunization campaigns. Misdiagnosis is plausible, especially in settings where diagnostic tools are limited and clinical expertise varies. Concerns surrounding gain‑of‑function research, biosafety gaps, and regional dual‑use research allegations highlight the importance of robust biosafety governance and independent diagnostic verification.
Ultimately, MLS in Bangladesh reflects a convergence of structural vulnerabilities, clinical ambiguity, and global biosecurity pressures. A comprehensive approach that integrates biosafety infrastructure, clinical evaluation, laboratory confirmation, and independent oversight is essential to accurately interpret MLS and restore public trust. Transparent investigation, strengthened biosafety.