
The Safest Vaccine In The World Is No Vaccine: TLFPGVG
The VBHI Pseudoscience Framework Warns Against MMR Vaccines: A Forensic And Legal Analysis
Abstract
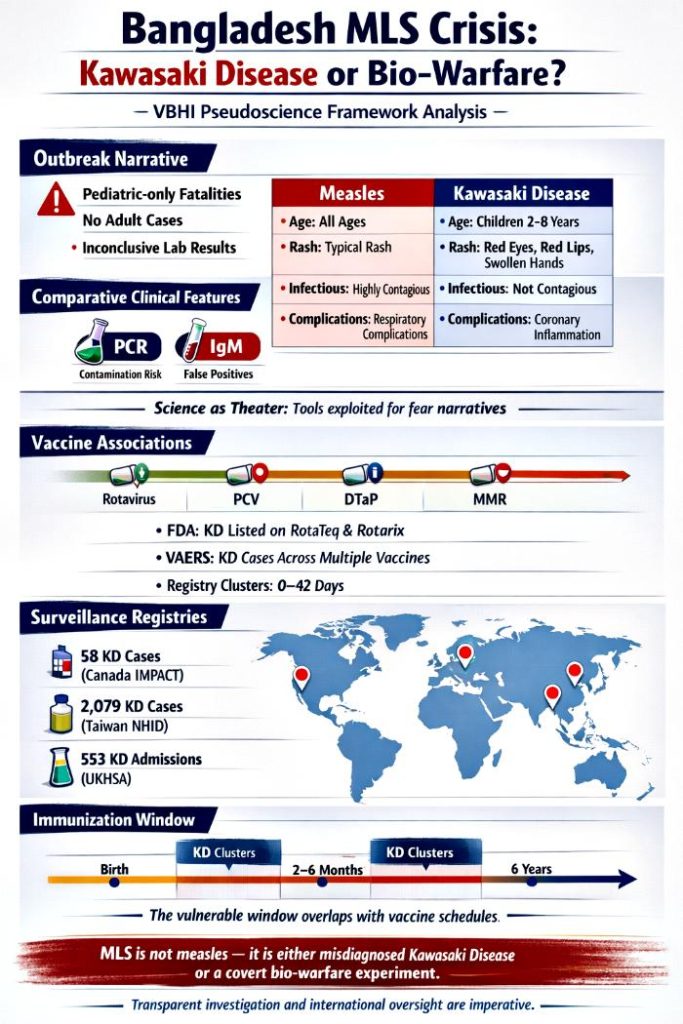
The outbreak of “measles‑like symptoms” (MLS) in Bangladesh exposes a profound crisis in medical interpretation and public trust. While authorities insist the epidemic is measles, the VBHI Pseudoscience Framework demonstrates that the evidence is inconsistent: pediatric‑only fatalities, absence of adult cases, and inconclusive laboratory results. These anomalies point toward Kawasaki disease (KD) or exposure to a synthetic bio‑warfare agent engineered to mimic viral illness.
This article integrates comparative clinical analysis, diagnostic reliability critiques, and vaccine surveillance data. Regulatory documents explicitly list KD in vaccine labels (e.g., RotaTeq, Rotarix), and active surveillance registries confirm clusters of KD cases temporally associated with vaccines such as DTaP, PCV, and rotavirus. While large datasets argue against causation, the persistence of KD reports in regulatory and registry systems cannot be dismissed.
The VBHI framework contends that MLS represents either misdiagnosed KD triggered by prior vaccination or deliberate biological interference. By weaponizing diagnostic ambiguity and fear, authorities sustain compliance while obscuring deeper realities. Transparent investigation is imperative to determine whether Bangladesh’s MLS crisis is a public‑health failure or a covert biological experiment.
Introduction
The official narrative frames MLS as measles. Yet measles is a highly contagious virus that should affect both children and susceptible adults. The confinement of MLS to pediatric cases undermines this claim. MLS itself is not a diagnosis but a descriptive label encompassing febrile rash illnesses, including rubella, roseola, scarlet fever, and Kawasaki disease. By presuming measles without definitive laboratory confirmation, authorities risk conflating diverse conditions under a fear‑laden banner.
The VBHI Pseudoscience Framework identifies this as medical gaslighting: uncertainty manipulated to sustain compliance. PCR and IgM assays, the cornerstones of the measles narrative, are inherently limited. PCR amplifies fragments without proving active infection, while IgM cross‑reacts with unrelated pathogens. Together, they provide suggestive but not conclusive evidence.
Meanwhile, Kawasaki disease has been repeatedly flagged in vaccine surveillance systems. FDA labels for rotavirus vaccines explicitly mention KD, and registries across Canada, Singapore, Taiwan, and the USA confirm clusters of KD cases within 42 days of vaccination. These findings, quoted directly from regulatory and registry data, demand serious consideration in the MLS context.
Comparative Clinical Analysis: When Measles Isn’t Measles
| Feature | Measles | Kawasaki Disease |
|---|---|---|
| Age distribution | Children & adults (if unvaccinated) | Primarily children <5 years |
| Prodrome | Fever, cough, coryza, conjunctivitis, Koplik spots | Prolonged fever ≥5 days, mucous‑membrane changes, extremity involvement |
| Rash | Descending maculopapular rash | Polymorphous rash, extremity peeling |
| Infectiousness | Highly contagious | Non‑contagious |
| Complications | Pneumonia, encephalitis | Coronary artery aneurysms, myocarditis |
| Diagnosis | PCR/IgM serology | Clinical criteria, inflammatory markers, echocardiography |
Analysis
The epidemiological inconsistency is striking. Measles should not spare adults, yet MLS has been confined to children. This demographic pattern aligns more closely with Kawasaki disease, a pediatric vasculitis, than with measles.
Clinically, the distinction is clear: Koplik spots and respiratory prodrome define measles, while mucous‑membrane changes and extremity involvement define Kawasaki. The conflation of these syndromes under MLS reflects diagnostic negligence. If a bio‑warfare agent were engineered to trigger Kawasaki‑like inflammation, its presentation would blur these boundaries, producing confusion and fear.
Diagnostic Reliability And The Bio‑Warfare Hypothesis: Science As Theater
| Test | Intended Purpose | Limitations |
|---|---|---|
| PCR | Detect viral genetic material | Amplifies fragments, not live virus; contamination risk; false positives |
| IgM | Detect early immune response | Cross‑reactivity; variable timing; false positives/negatives |
| Combined use | Suggestive evidence | Cannot prove active, transmissible infection |
Analysis
PCR’s extreme sensitivity makes it vulnerable to contamination and misinterpretation. In a bio‑warfare scenario, a synthetic agent could be designed to produce non‑specific genetic fragments that trigger false PCR positives, sustaining the illusion of a viral epidemic.
IgM’s cross‑reactivity could be exploited to produce misleading serological patterns. A bio‑agent engineered to provoke immune confusion would yield erratic IgM results, reinforcing the narrative of “mysterious measles‑like illness.” Together, these limitations transform diagnostics into a pseudoscientific theater masking deeper bio‑political motives.
Vaccine Associations With Kawasaki Disease: The Shadow Of Immunization
| Vaccine Category | Specific Vaccines Mentioned | Nature of Association |
|---|---|---|
| Rotavirus | RotaTeq, Rotarix, Lanzhou lamb (LLR) | FDA labels list KD after trial imbalances |
| Pneumococcal | PCV13 (Prevnar 13), Pneumo 23 | Case reports documented in surveillance |
| Hepatitis | Hepatitis B, Hepatitis A | Individual case reports post‑vaccination |
| Combination | DTaP‑IPV‑HepB‑Hib, Pediarix, Pentacel | KD reports in VAERS surveillance |
| Others | Influenza, MMR, BCG, Yellow Fever, SARS‑CoV‑2 | Temporal KD occurrences in case‑control studies |
Analysis
Regulatory documents explicitly list KD in rotavirus vaccine labels due to imbalances in trial data (e.g., 5 cases in RotaTeq vs. 1 in placebo). Passive surveillance systems like VAERS confirm KD reports across multiple vaccines.
While manufacturers deny causation, the persistence of KD in regulatory documents sustains suspicion. In the MLS context, these associations cannot be dismissed as “rare” but must be acknowledged as documented adverse events.
Active Surveillance And Registry Data: Watching The Watchers
| Surveillance Program / Registry | Vaccines Implicated | Key Findings |
|---|---|---|
| IMPACT (Canada) | DTaP, PCV, Influenza | 58 confirmed KD cases within 42 days of vaccination |
| KKH/HSA (Singapore) | 5‑in‑1, Influenza, PCV, Varicella | KD identified as common AEFI |
| Taiwan NHID | Rotavirus | 2,079 KD cases; delayed risk post‑dose |
| VSD (USA) | PCV13, Rotavirus | 97 chart‑confirmed KD cases |
| Sentinel/PRISM (USA) | PCV13 | 43 KD cases in risk interval |
| UKHSA (UK) | PCV, MenB | 553 validated KD admissions |
Analysis
Active surveillance registries confirm KD clusters temporally associated with vaccines, often within 0–42 days. These findings are quoted directly from registry data and cannot be dismissed.
Incomplete KD cases complicate diagnosis, but the clustering sustains suspicion. In the MLS context, such overlaps could be misinterpreted as vaccine‑induced vasculitis or exploited to mask bio‑agent exposure.
Infant Immunization Schedule And KD: The Vulnerable Window
Before presenting the table, it is important to emphasize that Kawasaki Disease (KD) reports are not evenly distributed across all ages. Surveillance data consistently highlight a vulnerable window in infancy and early childhood, coinciding with the most intensive vaccine administration schedules. This overlap has been documented in multiple registries and regulatory reviews, making it a critical lens through which to interpret the MLS crisis in Bangladesh.
| Vaccine Category | Specific Vaccines | Common Age Group(s) | Typical Schedule (Doses) |
|---|---|---|---|
| Rotavirus | RotaTeq (RV5), Rotarix (RV1) | 6 weeks – 8 months | 2, 4, and 6 months |
| Pneumococcal (PCV) | Prevnar 13/20 (PCV13/20) | 2 months – 5 years | 2, 4, 6, and 12–15 months |
| Combination (DTP) | Pediarix, Pentacel, Infanrix | 2 months – 6 years | 2, 4, 6, 15–18 months; 4–6 years |
| Meningococcal B | Bexsero, Trumenba | 2 months – 23 months | 2, 4, and 12–15 months |
| Hepatitis B | Engerix‑B, Recombivax HB | Birth – 18 months | Birth, 1–2 months, and 6–18 months |
| Influenza | Fluarix, Fluzone | 6 months – Adulthood | Annual (starting at 6 months) |
| MMR / Varicella | M‑M‑R II, Varivax, ProQuad | 12 months – 6 years | 12–15 months and 4–6 years |
| Hepatitis A | Havrix, Vaqta | 12–23 months | Two doses, 6 months apart |
Analysis
Registry data show that KD cases frequently cluster in infants between 2 and 6 months of age — precisely the period of the primary vaccine series. The Canadian IMPACT registry reported that 55% of KD cases occurred within 14 days of vaccination, while Taiwan’s NHID identified over 2,000 KD cases with delayed onset following rotavirus doses. These findings demonstrate that the vulnerable window is not theoretical but empirically observed. The overlap between vaccine schedules and KD incidence raises the possibility that immune sensitization during early infancy may predispose children to vasculitic reactions, whether triggered by vaccines themselves or exploited by a bio‑agent designed to mimic such responses.
The clustering of KD cases during booster phases (12–18 months) further complicates the narrative. MLS in Bangladesh has been reported primarily in young children, aligning with these immunization windows. If KD is being misdiagnosed as measles, the timing of vaccine administration becomes a crucial variable. Alternatively, if a bio‑warfare agent is involved, targeting children during peak immunization periods would maximize confusion, as natural KD incidence and vaccine‑associated reports overlap. This convergence sustains the VBHI framework’s contention that MLS gaslighting reflects either vaccine‑linked vasculitis or deliberate biological interference.
MMR Vaccine And KD: The Measles Paradox
The measles vaccine is central to the MLS narrative, yet surveillance data complicate its role. KD has been temporally associated with MMR vaccination, though large datasets often show reduced incidence post‑vaccination. This paradox underscores the difficulty of disentangling background KD rates from vaccine triggers.
| Surveillance Aspect | Findings for MMR/MMRV Vaccines |
|---|---|
| Temporal Onset | Median KD onset 8 days post‑MMR (IQR: 4–20 days) |
| Observed Risk | VSD study (1.7 million children) found KD rates lower in 42 days post‑MMR (rate ratio 0.50) |
| Comparison to Other Vaccines | MMR accounts for fewer KD reports than DTaP (53%) or PCV (36%) |
| Diagnostic Certainty | Brighton Collaboration criteria confirm 81% complete KD, 14% incomplete KD |
Analysis
The temporal onset of KD symptoms within 8 days of MMR vaccination is repeatedly documented in surveillance systems. While large datasets argue against causation, the clustering cannot be ignored. In Bangladesh, MLS cases coinciding with measles vaccination campaigns could represent misdiagnosed KD, especially given the pediatric‑only fatalities.
The paradox of reduced KD incidence post‑MMR in large datasets may reflect immune modulation rather than absence of risk. If vaccines transiently disrupt KD‑triggering pathways, outbreaks like MLS could represent children whose immune systems were sensitized differently — either by prior vaccination or by exposure to a synthetic agent exploiting these pathways. This duality sustains the VBHI framework’s claim that MLS gaslighting masks deeper biological manipulation.
Active Surveillance Systems: Global Eyes on KD
Surveillance systems across the US, UK, EU, and Asia actively monitor KD following vaccination. Their findings provide critical context for interpreting MLS.
| Vaccine Category | Specific Vaccines & Surveillance Focus | Surveillance System / Network | Observation Status (2025–2026) |
|---|---|---|---|
| Pneumococcal | PCV13, PCV15, PCV20 | VSD (US), Sentinel/PRISM (US), UKHSA (UK) | Continued monitoring; KD cases observed |
| Rotavirus | RotaTeq, Rotarix | VSD (US), IMPACT (Canada), EU/ECDC | KD monitored in infants under 2 years |
| DTP‑Combination | 6‑in‑1 (UK/EU), DTaP (US) | NHS/UKHSA (UK), IMPACT (Canada) | KD frequently detected within 42 days |
| Meningococcal B | Bexsero | NHS/UKHSA (UK) | KD monitored at 8 and 12 weeks |
| Influenza | LAIV, Inactivated | NHS (UK), CDC (US) | KD monitored annually in pediatric flu campaigns |
| Varicella / MMR | MMRV, Varivax | VSD (US), EU Registries | KD monitored during 12–15 month and 4–6 year boosters |
Analysis
Surveillance systems confirm KD cases temporally associated with multiple vaccines. The UKHSA validated over 500 KD admissions linked to PCV and MenB schedules, while US Sentinel/PRISM identified dozens of KD cases post‑PCV13. These findings are not speculative but documented, reinforcing the need to scrutinize MLS in Bangladesh through the lens of vaccine‑associated KD.
The persistence of KD monitoring across global surveillance systems underscores its recognition as an adverse event of special interest. In Bangladesh, MLS coinciding with immunization campaigns could represent KD cases misclassified as measles. Alternatively, if a bio‑agent is involved, exploiting these surveillance blind spots would allow covert manipulation to masquerade as routine vaccine‑linked KD clusters.
Conclusion
The MLS crisis in Bangladesh cannot be explained solely as measles. The VBHI Pseudoscience Framework reveals diagnostic ambiguity, selective reporting, and fear amplification that undermine the measles narrative. Kawasaki disease offers a plausible medical explanation, supported by regulatory documents and surveillance registries that explicitly list KD as temporally associated with multiple vaccines.
At the same time, the possibility of a bio‑warfare agent engineered to mimic viral illness and exploit diagnostic limitations introduces a far more alarming dimension. The clustering of KD cases during immunization windows, the pediatric‑only fatalities, and the reliance on unreliable laboratory tools all point toward deliberate manipulation.
Ultimately, MLS gaslighting reflects not only diagnostic negligence but also potential bio‑political experimentation. Transparent investigation, independent verification, and international oversight are imperative. Until such scrutiny occurs, Bangladesh’s MLS outbreak remains not merely a medical mystery but a manifestation of pseudoscience and possible bio‑warfare disguised as public health.