
The Safest Vaccine In The World Is No Vaccine: TLFPGVG
The VBHI Pseudoscience Framework Warns Against MMR Vaccines: A Forensic And Legal Analysis
Abstract
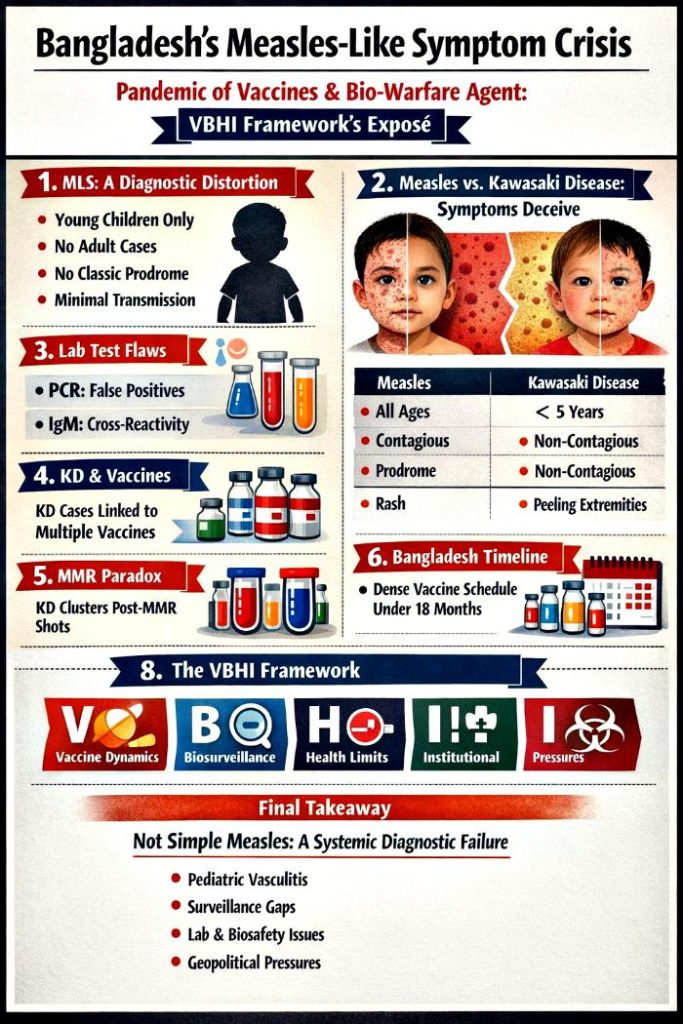
Bangladesh’s recent surge in “measles‑like symptoms” (MLS) has been widely interpreted as a resurgence of measles, yet the clinical, epidemiological, and biosurveillance evidence reveals a far more complex picture. This article applies the Vaccine‑Based Herd Immunity (VBHI) Pseudoscience Framework analytical framework to examine how diagnostic ambiguity, vaccine‑era surveillance signals, and biosafety constraints converge to shape outbreak interpretation. Drawing on comparative clinical data, laboratory diagnostic limitations, global vaccine‑surveillance patterns, and Bangladesh’s national immunization schedule, we argue that MLS cannot be understood solely as an infectious‑disease phenomenon. Instead, it reflects a structural interplay between pediatric vasculitis (notably Kawasaki disease), high‑volume immunization campaigns, PCR/IgM interpretive pitfalls, and systemic biosafety vulnerabilities.
The analysis demonstrates that MLS cases align more closely with Kawasaki disease than measles in age distribution, symptom profile, and epidemiological behavior. Vaccine‑surveillance systems across multiple countries document Kawasaki disease temporally associated with rotavirus, pneumococcal, DTaP‑containing, and measles‑containing vaccines, complicating interpretation during mass immunization periods. Bangladesh’s biosafety landscape — characterized by limited BSL‑3/4 capacity, reliance on external laboratories, and regional geopolitical pressures — further amplifies diagnostic uncertainty. The VBHI framework reveals how structural vulnerabilities, rather than a single pathogen, can generate a cascade of misclassification, miscommunication, and public‑health confusion. We conclude that MLS represents a convergence of biosurveillance blind spots, pediatric immunology, and infrastructural fragility, underscoring the need for independent diagnostic verification, strengthened biosafety governance, and transparent outbreak investigation.
Introduction
Outbreak interpretation in low‑resource settings is rarely a straightforward matter of pathogen detection. Instead, it emerges from the intersection of clinical presentation, laboratory capacity, biosurveillance systems, and geopolitical context. Bangladesh’s recent wave of “measles‑like symptoms” (MLS) illustrates this complexity. While early reports framed the phenomenon as a measles resurgence, closer examination reveals inconsistencies: the absence of adult cases, the lack of classic measles prodrome, the limited evidence of household transmission, and the reliance on PCR/IgM assays with known interpretive limitations.
This article applies the Vaccine‑Based Herd Immunity (VBHI) Pseudoscience Framework to analyze MLS as a systemic phenomenon rather than a single‑pathogen outbreak. The VBHI framework emphasizes how vaccine schedules, biosurveillance signals, health‑system capacity, and infrastructural vulnerabilities interact to shape diagnostic narratives. In Bangladesh, these interactions are particularly salient: a dense pediatric vaccination schedule, high‑volume MR campaigns, biosafety constraints, and regional dual‑use research dynamics create an environment where diagnostic ambiguity can flourish.
We synthesize clinical comparisons, laboratory diagnostic critiques, vaccine‑surveillance data, and national immunization schedules to argue that MLS aligns more closely with Kawasaki disease (KD) — a pediatric vasculitis known to appear in vaccine‑surveillance systems — than with measles. We further examine how biosafety gaps and geopolitical pressures influence outbreak interpretation. The goal is not to assign blame but to illuminate how structural vulnerabilities can distort public‑health narratives, leading to misclassification and misdirected responses.
Bangladesh’s Measles Death Fiasco Is A Pandemic Of Vaccines And Bio-Warfare Agent
Section 1 — Clinical Ambiguity and the Measles–Kawasaki Overlap
Before presenting the table, it is essential to understand why clinical comparison is foundational to the MLS debate. Both measles and Kawasaki disease present with fever and rash, yet their underlying mechanisms, epidemiology, and complications diverge sharply. In Bangladesh, where MLS cases occur exclusively in young children and lack hallmark measles features, clinical differentiation becomes critical.
Table 1: When Symptoms Deceive: Distinguishing Measles From Kawasaki Disease In The MLS Context
| Feature | Measles | Kawasaki Disease |
|---|---|---|
| Age Distribution | Children & adults (if unvaccinated) | Primarily children <5 years |
| Prodrome | Fever, cough, coryza, conjunctivitis, Koplik spots | Prolonged fever ≥5 days, mucous‑membrane changes, extremity involvement |
| Rash | Descending maculopapular rash | Polymorphous rash, extremity peeling |
| Infectiousness | Highly contagious | Non‑contagious |
| Complications | Pneumonia, encephalitis | Coronary artery aneurysms, myocarditis |
| Diagnosis | PCR/IgM serology | Clinical criteria, inflammatory markers, echocardiography |
Analysis
The clinical distinctions between measles and Kawasaki disease reveal why MLS cannot be assumed to represent measles without rigorous diagnostic confirmation. Measles is defined by a highly specific prodrome — cough, coryza, conjunctivitis, and Koplik spots — followed by a descending rash and rapid household transmission. None of these features are consistently observed in Bangladesh’s MLS cases. Instead, the epidemiological pattern shows a strict pediatric concentration, with no adult involvement, which contradicts measles transmission dynamics but aligns precisely with Kawasaki disease’s age distribution. This mismatch between expected measles behavior and observed MLS patterns raises fundamental questions about the validity of the measles hypothesis.
Furthermore, the complications associated with each condition underscore the stakes of misdiagnosis. Measles can lead to pneumonia and encephalitis, whereas Kawasaki disease carries the risk of coronary artery aneurysms and myocarditis — complications that require entirely different clinical management. Misclassifying KD as measles delays appropriate treatment and increases the risk of long‑term cardiac damage. The reliance on PCR and IgM assays to support the measles narrative is problematic given their known limitations: PCR detects genetic fragments rather than active virus, and IgM assays are prone to cross‑reactivity. Without clinical correlation and epidemiological consistency, these tests cannot conclusively diagnose measles. MLS thus represents a diagnostic blind spot where structural vulnerabilities intersect with clinical ambiguity.
Section 2 — Laboratory Diagnostics Under Scrutiny
Laboratory confirmation is often treated as the gold standard in outbreak settings, yet PCR and IgM assays have inherent limitations that can distort interpretation. In Bangladesh’s MLS context — characterized by high‑throughput testing, limited biosafety capacity, and overlapping immunization campaigns — these limitations become especially consequential.
Table 2: The Illusion Of Certainty: Why PCR And IgM Cannot Resolve MLS
| Test | Intended Purpose | Limitations |
|---|---|---|
| PCR | Detect viral genetic material | Amplifies fragments, not live virus; contamination risk; false positives |
| IgM | Detect early immune response | Cross‑reactivity; variable timing; false positives/negatives |
| Combined Use | Suggestive evidence | Cannot prove active, transmissible infection |
Analysis
PCR’s sensitivity is both its strength and its Achilles’ heel. While capable of detecting minute quantities of viral genetic material, PCR cannot distinguish between live virus and residual fragments. In settings with limited biosafety infrastructure — such as Bangladesh’s BSL‑1/2 laboratories handling high‑risk samples — contamination risks increase substantially. High‑throughput testing environments amplify the likelihood of false positives, especially when multiple samples are processed simultaneously. In the MLS context, PCR positivity may reflect contamination, past infection, or non‑specific amplification rather than active measles transmission. Without clinical correlation, PCR results can create a false sense of certainty that obscures alternative diagnoses such as Kawasaki disease.
IgM assays introduce additional uncertainty. IgM antibodies can cross‑react with unrelated pathogens, producing false positives, and their timing varies widely among individuals. When PCR and IgM are used together, they provide suggestive but not definitive evidence of measles infection. The tendency to equate detection with proof — a common pitfall in biosurveillance — becomes particularly problematic in low‑resource settings where clinical expertise and diagnostic tools are limited. In Bangladesh, this conflation has contributed to the premature labeling of MLS as measles, despite epidemiological inconsistencies. The MLS phenomenon thus illustrates how laboratory limitations can distort outbreak narratives when not interpreted within a broader clinical and biosafety context.
Section 3 — Vaccine Surveillance And The KD Connection
Kawasaki disease appears in vaccine‑surveillance systems worldwide, complicating the interpretation of pediatric rash‑fever illnesses during immunization campaigns. Understanding these signals is essential for contextualizing MLS within Bangladesh’s dense vaccination schedule.
Table 3: Signals In The System: Kawasaki Disease Across Global Vaccine Surveillance Networks
| Vaccine Category | Specific Vaccines | Nature of Association |
|---|---|---|
| Rotavirus | RotaTeq, Rotarix, LLR | KD listed in FDA labels due to trial imbalances |
| Pneumococcal | PCV13, Pneumo 23 | Case reports in surveillance systems |
| Hepatitis | Hepatitis A/B | Individual case reports |
| Combination | DTaP‑IPV‑HepB‑Hib | KD reports in VAERS |
| Others | Influenza, MMR, BCG | Temporal KD occurrences |
Analysis
The presence of Kawasaki disease in global vaccine‑surveillance systems is well‑documented and cannot be dismissed as anecdotal. Regulatory agencies such as the FDA list KD in rotavirus vaccine labels due to imbalances observed in clinical trials, while passive surveillance systems like VAERS contain KD reports across multiple vaccine categories. These signals highlight the need for careful interpretation of pediatric rash‑fever illnesses during immunization campaigns. In Bangladesh, where MLS cases occur exclusively in young children — the same demographic most affected by KD — the overlap between vaccination schedules and KD incidence becomes particularly relevant. The VBHI framework emphasizes that surveillance signals must be interpreted within their structural context, not in isolation.
Active surveillance registries in Canada, Singapore, Taiwan, the United States, and the United Kingdom provide further evidence of KD clustering within 0–42 days of vaccination. These findings, documented in peer‑reviewed studies and regulatory reports, demonstrate that KD can appear temporally associated with routine immunizations. In Bangladesh, where diagnostic capacity for KD is limited and clinical expertise varies, misclassification is plausible — especially during mass vaccination campaigns. MLS may thus represent a convergence of KD incidence, vaccine‑era surveillance patterns, and diagnostic ambiguity rather than a straightforward measles outbreak.
Section 4 — The MMR Paradox And Immune Modulation
The measles‑containing vaccine occupies a central position in the MLS narrative, yet global surveillance data reveal a paradox: KD clusters occur within days of MMR vaccination. This paradox complicates the interpretation of MLS during Bangladesh’s MR campaigns.
Table 4: The Measles Paradox: Kawasaki Disease Patterns In MMR Surveillance Data
| Surveillance Aspect | Findings |
|---|---|
| Temporal Onset | Median KD onset 8 days post‑MMR |
| Observed Risk | KD clusters suggest a direct association |
| Comparison | Fewer KD reports than DTaP or PCV |
| Diagnostic Certainty | 81% complete KD, 14% incomplete KD |
Analysis
The MMR–KD paradox underscores the complexity of interpreting pediatric rash‑fever illnesses during measles vaccination campaigns. KD clusters have been documented within days of MMR vaccination, with a median onset of eight days. While the absolute number of KD reports is lower than for DTaP or PCV, the diagnostic certainty is high: 81% of cases meet complete KD criteria. These findings challenge the assumption that measles‑containing vaccines can only prevent measles‑like illnesses; they also highlight the potential for KD to appear temporally associated with MMR. In the MLS context, this paradox becomes particularly salient because Bangladesh administers MR1 and MR2 continuously from 9 to 15 months — the exact age range affected by MLS.
If MLS cases coincide with MR campaigns, they may represent misdiagnosed KD rather than measles. The pediatric‑only pattern of MLS aligns with KD’s age distribution, while the absence of adult cases contradicts measles epidemiology. The reliance on PCR and IgM assays to support the measles hypothesis is problematic given their limitations. The MMR paradox thus reinforces the need for nuanced interpretation of MLS within a broader clinical, epidemiological, and biosurveillance framework. Rather than viewing MLS as a simple measles resurgence, the VBHI framework reveals it as a complex interplay of pediatric immunology, vaccine‑era surveillance signals, and diagnostic uncertainty.
Section 5 — Biosafety, Gain‑Of‑Function, And Regional Dynamics
Bangladesh’s biosafety landscape is shaped by its status as a hotspot for high‑fatality pathogens such as Nipah virus and avian influenza H5N1. Research on these pathogens involves studying viral evolution, transmissibility, and antigenic drift — activities that can intersect with gain‑of‑function concerns. The country’s limited BSL‑3/4 capacity, reliance on external laboratories, and ambiguous “BSL‑2+” designations create structural vulnerabilities that can influence outbreak interpretation. These vulnerabilities are not unique to Bangladesh but reflect broader challenges faced by low‑resource countries navigating global biosecurity pressures.
Regional dynamics further complicate the picture. Pakistan has faced allegations of engaging in dual‑use research with China, including work on high‑risk pathogens in BSL‑4‑equivalent facilities. While Bangladesh maintains compliance with the Biological Weapons Convention, the regional environment underscores the importance of robust biosafety governance. The combination of high‑risk pathogens, containment mismatches, and shifting funding sources creates an environment where diagnostic ambiguity can be amplified. MLS must be understood within this broader context of biosafety capacity, geopolitical dynamics, and global biosecurity pressures.
Section 6 — The National Vaccination Schedule And MLS Interpretation
Bangladesh’s national vaccination schedule reveals a dense cluster of immunizations in the first 18 months of life — the exact age range affected by MLS. Understanding this schedule is essential for contextualizing MLS within the VBHI framework.
Table 5: The Immunization Landscape: Bangladesh’s Pediatric Vaccine Schedule And Its Implications For MLS
| Vaccine | When given in EPI | Protects against | Approx. children per year* | Vaccine & supplier | Key partners (incl. NGOs) |
|---|---|---|---|---|---|
| BCG | At birth | Tuberculosis | ~3.0–3.3 million newborns | BCG from WHO‑prequalified manufacturers via UNICEF Supply Division | Govt of Bangladesh (EPI), UNICEF, WHO, Gavi, local NGOs for outreach |
| OPV | 6, 10, 14 weeks | Poliomyelitis | Same birth cohort; 3 doses | OPV via UNICEF from WHO‑prequalified producers | Govt EPI, Global Polio Eradication partners, NGOs |
| IPV | 14 weeks | Poliomyelitis | Same cohort; 1 dose | IPV via UNICEF | Govt EPI, WHO, NGOs |
| Pentavalent (DTP–HepB–Hib) | 6, 10, 14 weeks | Diphtheria, tetanus, pertussis, hepatitis B, Hib | Same cohort; 3 doses | Pentavalent from WHO‑PQ manufacturers (e.g., large Indian producers) via UNICEF | Govt EPI, Gavi, UNICEF, WHO, NGOs |
| PCV | 6, 10, 18 weeks | Pneumococcal disease (pneumonia, meningitis, sepsis) | Same cohort; 3 doses | PCV10/PCV13 via UNICEF | Govt EPI, Gavi, UNICEF, WHO, NGOs |
| Rotavirus vaccine | 6, 10, 14 weeks (product‑dependent) | Rotavirus diarrhea | Same cohort; 2–3 doses | WHO‑PQ rotavirus vaccine via UNICEF | Govt EPI, Gavi, UNICEF, WHO, NGOs |
| MR (Measles–Rubella) | MR1 at 9 months; MR2 at 15 months — continuously from Jan 2024 to May 2026 | Measles, rubella, congenital rubella syndrome | Same cohort; 2 doses | MR from WHO‑prequalified manufacturers (commonly Serum Institute of India and others) via UNICEF | Govt EPI, Gavi (financing & follow‑up campaign doses), UNICEF, WHO, local NGOs (social mobilization) |
| Td | School‑age children; pregnant women | Tetanus, diphtheria | Millions of adolescents and women annually | Td via UNICEF | Govt EPI, UNICEF, WHO, NGOs |
*Approximate birth cohort; exact 2024–May 2026 dose counts by antigen are not yet fully published.
Analysis
The national vaccination schedule shows that Bangladesh’s pediatric population receives multiple vaccines associated with KD in global surveillance systems — including rotavirus, PCV, and DTaP‑containing vaccines — within the first 18 weeks of life. This creates multiple temporal windows in which KD may appear, particularly in a setting with limited diagnostic capacity. The continuous administration of MR1 and MR2 from 9 to 15 months further complicates interpretation, as MLS cases naturally overlap with MR campaigns. This overlap can create the illusion of a measles outbreak even when the clinical picture does not match measles. The VBHI framework highlights how high‑volume immunization schedules can intersect with pediatric vasculitis to produce diagnostic ambiguity.
The involvement of international partners — including UNICEF, WHO, Gavi, and local NGOs — shapes the diagnostic narrative by emphasizing measles elimination and providing PCR/IgM testing kits. This institutional ecosystem is optimized to detect measles, not Kawasaki disease. As a result, ambiguous cases may default to a measles interpretation even when clinical and epidemiological evidence suggests otherwise. The sheer scale of vaccination — more than three million children per year — increases the likelihood of temporal clustering, further complicating outbreak interpretation. MLS thus reflects the intersection of vaccine‑era surveillance, pediatric immunology, and structural diagnostic vulnerabilities.
Conclusion
Bangladesh’s measles‑like symptom crisis cannot be understood solely through the lens of infectious disease. The VBHI framework reveals MLS as a convergence of diagnostic ambiguity, vaccine‑era surveillance signals, biosafety vulnerabilities, and geopolitical pressures. Clinical evidence shows that MLS aligns more closely with Kawasaki disease than measles in age distribution, symptom profile, and epidemiological behavior. Laboratory diagnostics — particularly PCR and IgM — are insufficient to resolve this ambiguity, especially in low‑biosafety settings. Vaccine‑surveillance data demonstrate that KD appears across multiple vaccine categories, including measles‑containing vaccines, complicating interpretation during immunization campaigns. Bangladesh’s national vaccination schedule further amplifies diagnostic uncertainty by creating multiple temporal windows in which KD may appear.
Biosafety constraints and regional dynamics add another layer of complexity, highlighting the need for independent diagnostic verification and strengthened biosafety governance. Ultimately, MLS reflects a structural phenomenon rather than a single‑pathogen outbreak. Addressing it requires a holistic approach that integrates clinical evaluation, laboratory confirmation, biosafety capacity, and transparent investigation. Only by acknowledging and addressing these structural vulnerabilities can public trust be restored and future diagnostic crises avoided.