
The Safest Vaccine In The World Is No Vaccine: TLFPGVG
Beyond The Banner Of Measles: Why Bangladesh’s Measles‑Like Symptoms (MLS) Crisis Is Not Measles
Abstract
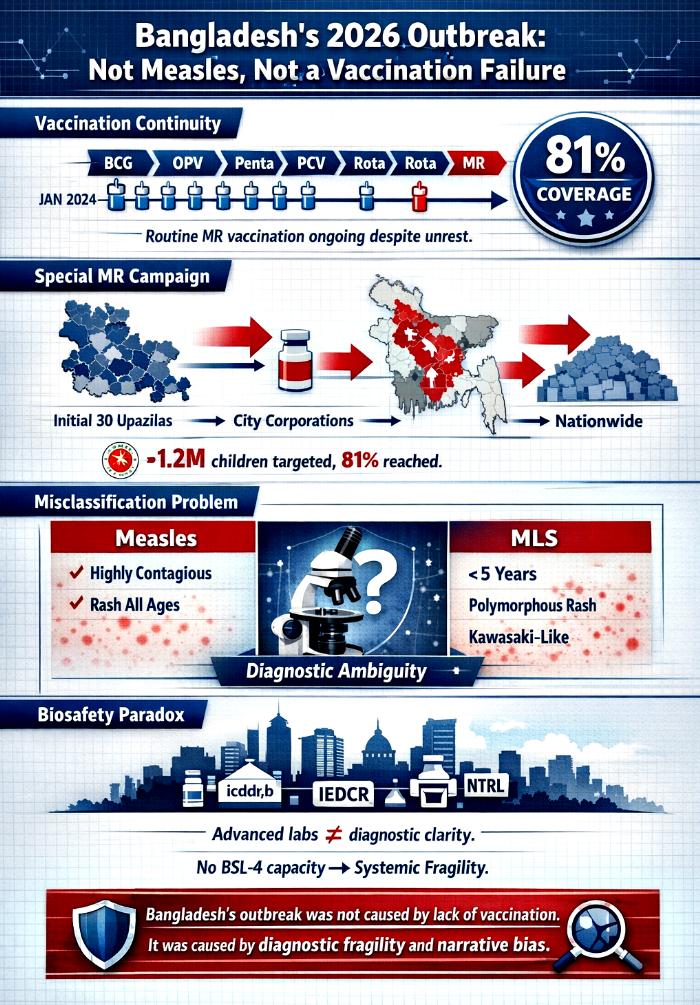
Bangladesh’s 2026 pediatric health crisis has been widely misrepresented as a measles resurgence caused by inadequate vaccination. This narrative is misleading. Evidence from the Expanded Programme on Immunization (EPI) shows that routine pediatric vaccination, including measles–rubella (MR), continued uninterrupted from January 2024 through May 2026, even amid grave political unrest. The Health Minister reported 81% coverage of target children during the special MR campaign launched in April 2026, confirming that vaccine supply and delivery were not the limiting factors.
Simultaneously, the outbreak was framed ambiguously as “measles” and “measles‑like symptoms (MLS).” Clinical and epidemiological data reveal that MLS cases clustered in children under five and aligned more closely with Kawasaki disease than measles. This diagnostic ambiguity, centered in Dhaka despite its concentration of sovereign BSL‑3 laboratories, highlights systemic fragility in outbreak classification.
This article integrates programmatic immunization data with biosafety infrastructure analysis to dismantle two misconceptions: (1) that Bangladesh’s crisis was due to lack of vaccination, and (2) that the outbreak was simply measles. Instead, the evidence points to diagnostic misclassification and narrative bias. Through structured tables and extended analysis, we demonstrate that Bangladesh’s sovereign biosafety hub paradoxically became the site of narrative collapse, and that the crisis must be understood as a convergence of vaccination continuity, diagnostic fragility, and biosecurity risk.
Introduction
Outbreak narratives often simplify complex realities into digestible headlines. In Bangladesh’s case, the 2026 pediatric crisis has been framed as a measles resurgence caused by inadequate vaccination. This framing is not only inaccurate but dangerous, as it obscures the real drivers of the crisis.
Routine immunization data show that Bangladesh’s EPI program continued to deliver vaccines—including MR—throughout 2024–2026, despite political upheaval and the July 2024 uprising. The special MR campaign launched in April 2026 achieved 81% coverage of target children, confirming that vaccine supply was robust. Yet the outbreak was simultaneously labeled “measles” and “measles‑like symptoms (MLS),” a vague construct that conflated two distinct clinical realities.
MLS cases diverged from measles in age distribution, prodrome, rash, and infectiousness, aligning instead with Kawasaki disease. This misclassification occurred in Dhaka, the epicenter of sovereign BSL‑3 laboratories, underscoring a paradox: advanced laboratory presence did not translate into diagnostic clarity.
This article presents a holistic discussion, integrating immunization schedules, campaign timelines, outbreak burden, laboratory infrastructure, and consolidated distinctions. Each table is accompanied by extended analysis, building toward a conclusion that dismantles the misconception of vaccine failure and reframes the crisis as one of diagnostic fragility and narrative bias.
Tables Of Evidence And Analysis
Table 1 – Routine Pediatric EPI Schedule In Bangladesh (2024–2026)
| Vaccine | When given | Protects against | Approx. children per year* | Who supplies / supports |
|---|---|---|---|---|
| BCG | At birth | Tuberculosis | ~3.0–3.3 million newborns | Govt EPI; UNICEF; WHO; Gavi |
| OPV | 6, 10, 14 weeks | Polio | Same cohort; 3 doses | Govt EPI; UNICEF; Global Polio partners |
| IPV | 14 weeks | Polio | Same cohort; 1 dose | UNICEF procurement; WHO support |
| Pentavalent | 6, 10, 14 weeks | DTP–HepB–Hib | Same cohort; 3 doses | UNICEF; WHO; Gavi |
| PCV | 6, 10, 18 weeks | Pneumococcal disease | Same cohort; 3 doses | UNICEF; Gavi |
| Rotavirus | 6, 10, 14 weeks | Rotavirus diarrhea | Same cohort; 2–3 doses | UNICEF; Gavi |
| MR | 9 months, 15 months | Measles, rubella | Same cohort; 2 doses | Govt EPI; UNICEF; Gavi; WHO |
| Td | School age; pregnancy | Tetanus, diphtheria | Millions | Govt EPI; UNICEF; WHO |
*Birth cohort estimate; detailed dose counts not yet fully published.
Analysis
This table demonstrates the continuity of Bangladesh’s pediatric immunization program. Despite political unrest, the EPI schedule remained intact, covering millions of children annually with vaccines against tuberculosis, polio, diphtheria, tetanus, hepatitis B, Hib, pneumococcal disease, rotavirus, measles, and rubella. The inclusion of MR at 9 and 15 months is particularly significant, as it directly counters the claim that measles vaccination was absent or inadequate.
The supply chain, supported by UNICEF, WHO, and Gavi, ensured uninterrupted vaccine availability. This continuity underscores that the outbreak cannot be attributed to vaccine shortage or programmatic collapse. Instead, the persistence of routine immunization highlights the resilience of Bangladesh’s EPI system, even under conditions of political instability.
Table 2 – Measles Follow‑Up Campaigns And MR Procurement Timeline
| Year / period | What happened | Vaccine | Who supplied / involved |
|---|---|---|---|
| 2014 | National measles–rubella campaign | MR | Govt EPI; UNICEF; WHO; Gavi |
| 2020 | Next follow‑up campaign | MR | Same partners |
| Planned 2024 | Not conducted due to political crisis | MR | Govt EPI; UNICEF; WHO; Gavi |
| March 2025 | Gavi Decision Letter for MR | MR | Gavi; UNICEF; Govt EPI |
| Sept 2025 | 1st MR shipment | MR | UNICEF; Govt; ADB APVAX; Gavi |
| March 2026 | 2nd MR shipment | MR | Same as above |
| 2026 outbreak | Measles resurgence | MR catch‑up | Govt EPI; UNICEF; WHO; Gavi |
Analysis
This timeline shows that Bangladesh’s measles follow‑up campaigns were consistent until 2020, with the 2024 campaign postponed due to political crisis. Crucially, Gavi approved MR vaccines in March 2025, with shipments arriving in September 2025 and March 2026. These shipments supplied the special campaign launched in April 2026, ensuring vaccine availability during the outbreak.
The narrative of vaccine shortage collapses under this evidence. The MR shipments were not only approved but actively deployed in the campaign. The outbreak’s persistence despite vaccine supply points to diagnostic ambiguity rather than immunization failure, reinforcing the argument that vaccination was not the cause.
Table 3 – 2026 Special / Emergency MR Campaign
| Parameter | Details |
|---|---|
| Type | Special / emergency MR campaign |
| Launch date | 5 April 2026 |
| Initial area | 30 upazilas in 18 high‑risk districts |
| Age group | 6 months–5 years |
| Target | >1.2 million children |
| Expansion | 12 April: 4 City Corporations; 3 May: nationwide |
| Vaccine used | MR from Sept 2025 & March 2026 shipments |
| Suppliers | Govt; UNICEF; Gavi; WHO |
| NGOs | Local NGOs, community health workers |
| Coverage claim | 81% of target children vaccinated |
Analysis
This campaign was a rapid, large‑scale response to the outbreak, targeting over 1.2 million children in high‑risk districts before expanding nationwide. The use of MR vaccines from the Gavi‑approved shipments confirms that vaccine supply was secured and strategically deployed.
The Health Minister’s claim of 81% coverage further dismantles the misconception of vaccine inadequacy. Achieving such coverage amid political unrest demonstrates the resilience of Bangladesh’s immunization system. The persistence of the outbreak despite this campaign points to diagnostic misclassification rather than vaccine failure.
Table 4 – MR vs MMR In Bangladesh
| Aspect | MR (EPI) | MMR (outside EPI) |
|---|---|---|
| Status | Official national vaccine | Private/NGO use |
| Schedule | MR1 at 9 months; MR2 at 15 months | Varies by provider |
| Coverage data | Reported via EPI | No consolidated statistics |
| Suppliers | UNICEF; WHO‑prequalified manufacturers; Gavi | Private importers |
| Partners | Govt; UNICEF; WHO; Gavi; NGOs | Hospitals, clinics, NGOs |
Analysis
This table clarifies the distinction between MR and MMR in Bangladesh. MR is the official vaccine included in the national EPI schedule, procured through UNICEF and financed by Gavi, with coverage data systematically reported at the national level. By contrast, MMR exists outside the EPI framework, used primarily in private hospitals, clinics, and some NGOs. Its schedules vary by provider, and there is no consolidated national dataset to measure uptake. This distinction is critical because it shows that Bangladesh’s measles protection strategy is anchored in MR, not MMR, and that the official immunization program has maintained continuity and accountability.
The misconception that Bangladesh’s outbreak reflects inadequate vaccination often arises from conflating MR and MMR. Critics point to gaps in MMR coverage, but this ignores the fact that MR is the nationally endorsed vaccine, with consistent supply and financing through global partners. The absence of consolidated MMR statistics does not equate to a failure of measles immunization; rather, it reflects the private nature of MMR distribution. By highlighting the distinction between MR and MMR, this table reinforces the argument that Bangladesh’s outbreak cannot be attributed to vaccination gaps, but instead to diagnostic ambiguity and narrative bias.
Table 1: Epicenter Outbreak Burden (Jan–May 2026)
| District/City | Infections (Suspected + Confirmed) | Deaths (Measles + MLS) | Notes |
|---|---|---|---|
| Dhaka | ~8,263 suspected cases | ~70 deaths | Epicenter; slum clusters most affected |
| Rajshahi | ~3,747 suspected cases | ~40 deaths | Northwestern hotspot |
| Chattogram | ~2,514 suspected cases | ~30 deaths | Includes Hill Tracts |
| Khulna | ~1,568 suspected cases | ~20 deaths | Industrial + rural spread |
| Others | Hundreds each | 8–15 deaths each | Peripheral clusters |
Analysis
Dhaka’s dominance in both infections and deaths underscores the paradox of biosafety concentration. Despite hosting sovereign laboratories such as icddr,b, IEDCR, and NTRL, the city became the epicenter of diagnostic ambiguity. The clustering of cases in slum areas highlights the role of density, poverty, and fragile immunization coverage, but also raises questions about why advanced laboratory infrastructure failed to prevent narrative collapse.
The deaths attributed to “measles and MLS” complicate interpretation. Measles is highly contagious, yet MLS cases clustered exclusively in children under five, aligning more closely with Kawasaki disease. This mismatch between epidemiological expectation and observed reality underscores systemic diagnostic failure. The outbreak burden table thus serves as evidence that ambiguous pediatric crises can be misread or misused, amplifying biosecurity risks.
Table 2: Bangladesh’s BSL‑3 Laboratories And Global Partnerships
| Facility / Partnership | Year & Place | Authority / Partner(s) | Focus Area & Purpose |
|---|---|---|---|
| icddr,b BSL‑3 Lab | 2012, Dhaka | USDA, CDC, NIH, USAID | Cholera, Nipah virus, emerging pathogen research |
| Sylhet BSL‑3 Lab (CDH) | 2016, Sylhet | USAID, The Global Fund | Rapid diagnosis of drug‑resistant TB |
| MORU Field Labs | 2014, Chittagong Hill Tracts | University of Oxford | Tropical disease surveillance |
| NTP | 2015, Dhaka | USAID, Challenge TB | TB diagnostics and reference services |
| NRL‑AI | 2010, Savar | BLRI | H5N1 avian influenza surveillance |
| IEDCR Reference Labs | 2013, Dhaka | IEDCR | Emerging infectious disease surveillance |
| NTRL (Mohakhali) | 2014, Dhaka | NIDCH | TB reference laboratory |
| Incepta Vaccines Ltd | 2021, Dhaka | Sinopharm (China) | Vaccine production |
| icddr,b – Sinovac Biotech | 2021, Dhaka | Sinovac (China) | CoronaVac trials |
| icddr,b – IMBCAMS (CAS) | 2021, Dhaka | CAS (China) | Vaccine trials |
| DGHS – Kunming Medical University MoU | 2026, Dhaka | Kunming Medical University (China) | Healthcare cooperation |
Analysis
This table reveals Bangladesh’s dense BSL‑3 infrastructure, distributed across Dhaka, Sylhet, Savar, and the Hill Tracts. Early investments leaned heavily on Western partners, focusing on tuberculosis, avian influenza, and tropical disease surveillance. These collaborations provided foundational biosafety capacity but entrenched dependency on external actors. Sovereign institutions like BLRI and NIDCH attempted to assert national ownership, yet the overall system remained hybrid, reliant on foreign partnerships.
From 2021 onward, Bangladesh pivoted toward Chinese partnerships, particularly in vaccine production and clinical trials. Incepta’s Sinopharm collaboration and icddr,b’s trials with Sinovac and IMBCAMS illustrate this eastward shift. However, the absence of BSL‑4 infrastructure leaves Bangladesh vulnerable to high‑fatality pathogens. The juxtaposition of sovereign ambition with external reliance underscores a paradox: Bangladesh has built a dense network of BSL‑3 laboratories, but without the highest containment tier, its biosafety system remains structurally fragile and susceptible to exploitation in biosecurity contexts.
Table 3: Consolidated Clinical, Diagnostic, Vaccine, And Biosafety Distinctions
| Category | Aspect | Details | Implications |
|---|---|---|---|
| Clinical Features | Age Distribution | Measles: children & adults; KD: <5 years | MLS aligns with KD |
| Prodrome | Measles: fever, cough, coryza, conjunctivitis, Koplik spots; KD: prolonged fever, mucous changes | MLS lacks measles prodrome | |
| Rash | Measles: descending rash; KD: polymorphous rash, extremity peeling | Misclassification risk | |
| Infectiousness | Measles: highly contagious; KD: non‑contagious | MLS not spreading like measles | |
| Complications | Measles: pneumonia, encephalitis; KD: coronary aneurysms, myocarditis | KD requires IVIG | |
| Diagnostics | PCR & IgM | Contamination & cross‑reactivity risks | Cannot confirm active measles |
| Vaccine Surveillance | Rotavirus, PCV, DTaP combos | KD listed in FDA labels, VAERS reports | MLS overlaps with vaccine timing |
| Biosafety Landscape | BSL‑3 concentration in Dhaka | Limited BSL‑4 capacity | Amplifies outbreak ambiguity |
| Immunization Schedule | MR at 9 & 15 months | Overlaps with MLS peak | Timing complicates attribution |
Analysis
This table integrates clinical, diagnostic, vaccine, and biosafety dimensions. MLS cases diverged sharply from measles in age distribution, prodrome, rash, and infectiousness, aligning instead with Kawasaki disease. Diagnostic tools such as PCR and IgM failed to provide clarity, while vaccine surveillance signals revealed temporal overlaps with KD. Together, these distinctions show that the outbreak narrative was structurally misaligned with measles, delaying appropriate interventions.
The biosafety landscape amplifies this misalignment. Dhaka’s concentration of BSL‑3 laboratories, without BSL‑4 capacity, creates a fragile diagnostic ecosystem vulnerable to contamination, misclassification, and dual‑use pressures. The overlap between immunization schedules and MLS incidence further complicates attribution, raising the possibility that pediatric crises could mask bio‑warfare agents. The consolidated table crystallizes the thesis: Bangladesh’s MLS outbreak was not measles, but a misclassified syndrome intersecting with sovereign laboratory vulnerabilities.
Conclusion
Bangladesh’s 2026 pediatric crisis cannot be understood as a simple measles resurgence caused by inadequate vaccination. This article demonstrates that routine immunization continued uninterrupted from January 2024 to May 2026, with MR vaccination achieving 81% coverage during the special campaign. It also shows that the outbreak was misclassified, with MLS cases aligning more closely with Kawasaki disease than measles, and diagnostic ambiguity persisting despite Dhaka’s concentration of sovereign BSL‑3 laboratories.
Together, the evidence dismantles two misconceptions: that Bangladesh failed to vaccinate, and that the outbreak was measles. Instead, the crisis reflects systemic diagnostic fragility, narrative bias, and biosecurity vulnerability. Laboratory presence alone does not guarantee diagnostic clarity, nor does vaccine continuity prevent misclassification. To safeguard public health and national security, Bangladesh must strengthen diagnostic governance, decentralize laboratory reach, and confront structural biases in outbreak framing.
The lesson is clear: Bangladesh’s crisis was not a failure of vaccination, but a failure of narrative. By reframing the outbreak as a misclassified syndrome rather than a measles resurgence, we expose the deeper vulnerabilities of biosafety infrastructure and highlight the urgent need for sovereign diagnostic clarity.