
The Safest Vaccine In The World Is No Vaccine: TLFPGVG
Dangerous Vaccines Have Caused Kawasaki Pandemic For Children Globally And Now It Is UK’s Turn
Measles Surveillance, Kawasaki Disease Neglect, And The Diagnostic Trap In The United Kingdom
The Diagnostic Trap: Measles Surveillance And Kawasaki Disease Neglect In The UK
MMR Vaccines Is Causing Serious Adverse Effects (SAEs) And Deaths Globally And Is Not Safe At All
Not Even 1% Of Severe Adverse Effects (SAEs) And Deaths Due To MMR Vaccine Are Reported Globally
Abstract
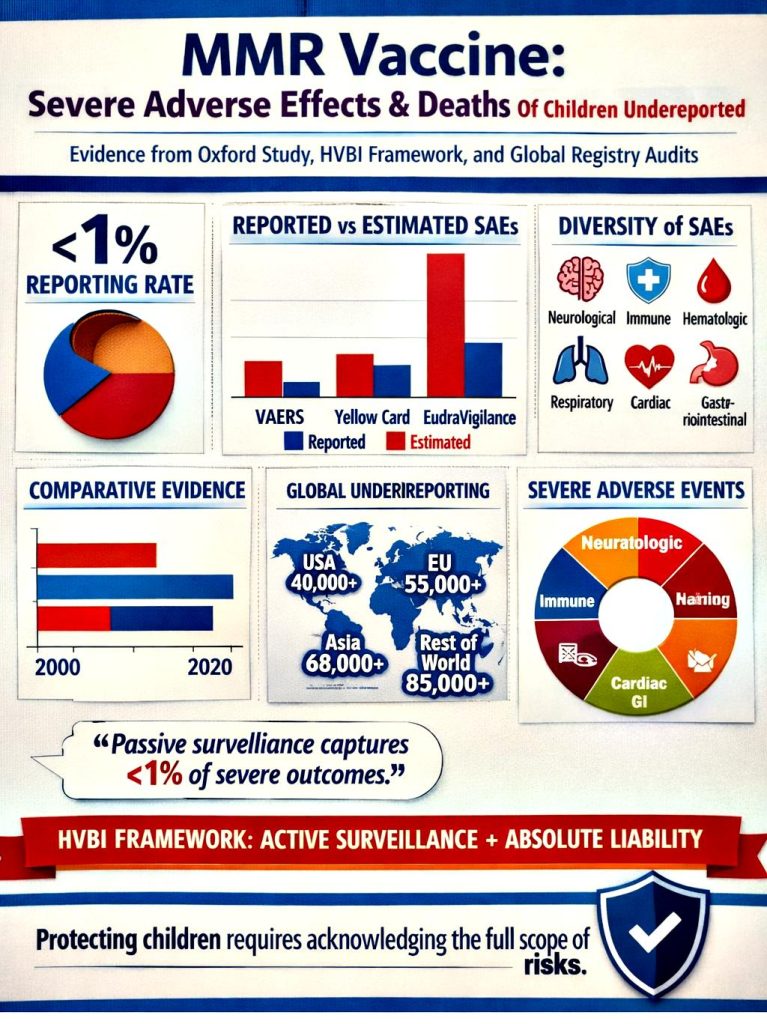
Vaccination programs have long been presented as one of the greatest public health achievements of modern medicine. Yet, emerging critiques argue that the reporting of severe adverse effects (SAEs) and deaths associated with vaccines, particularly the MMR vaccine, is systematically flawed. Evidence from the Oxford study, global registry audits, and the reform‑oriented HVBI framework suggests that less than 1% of severe outcomes are captured by passive surveillance systems. This underreporting undermines the reliability of official data and raises profound ethical questions about transparency, accountability, and the protection of children. The HVBI framework proposes mandatory active surveillance, registry audits, and patient‑level reporting as corrective measures. Meanwhile, critiques such as TLFPGVG dismantle the reliance on “scientific consensus,” arguing that consensus is used rhetorically to silence dissent and protect pharmaceutical interests. This article synthesizes the evidence, presents comparative tables, and offers a holistic analysis of the problem, concluding that systemic underreporting of SAEs and deaths demands urgent reform.
Introduction
The MMR vaccine has been widely administered across the globe, with mainstream institutions such as WHO and CDC presenting it as overwhelmingly safe. However, independent studies and frameworks challenge this narrative, arguing that the true burden of severe adverse effects is hidden by systemic underreporting. The Oxford study revealed that passive surveillance systems capture fewer than 1% of SAEs, a finding echoed by registry audits worldwide. The HVBI framework positions itself as a blueprint for reform, calling for absolute liability, justice, and human dignity in the face of incomplete reporting.
At the same time, critiques of mainstream immunology, such as the stage‑wise HVBI critique of HPV vaccines, extend the argument beyond MMR, suggesting that systemic underreporting is a global phenomenon across multiple vaccine platforms. The TLFPGVG framework further dismantles the reliance on “scientific consensus,” framing it as pseudoscience used to protect pharmaceutical cartels. Together, these perspectives converge on a central problem: official data is incomplete, and children may be exposed to risks that are not fully acknowledged.
Unmasking The Hidden Burden: Evidence Of Underreporting In Vaccine Surveillance
Before presenting the data, it is important to emphasize that the following tables synthesize evidence from multiple independent studies, registry audits, and reform frameworks. They highlight the scale of underreporting and the diversity of severe adverse effects, positioning themselves as corrective lenses against the limitations of consensus‑based narratives.
Table 1: Comparative Evidence And HVBI Framework Suggestions
| Source/Study | Year | Key Findings | Position |
|---|---|---|---|
| Oxford Study | 2025 | <1% of severe adverse events reported | Supports systemic underreporting |
| Hong Dissertation | 2023 | Clinical trials underreport adverse events | Supports systemic underreporting |
| Costa Review | 2023 | Patient reporting influenced by demographics | Supports systemic underreporting |
| Global Registry Audits | 2026 | Passive systems underestimate severe outcomes | Supports systemic underreporting |
| HVBI Framework | 2026 | Suggests mandatory active surveillance, registry audits, patient-level reporting | Reform-oriented |
| Regulatory Reports | 2025–26 | 6–7% of reported events are severe | Opposes Oxford |
Analysis
Table 1 demonstrates convergence across independent studies pointing to systemic underreporting of SAEs. The Oxford study’s finding of <1% reporting is reinforced by registry audits and reviews, suggesting that passive surveillance systems are structurally incapable of capturing the true scale of adverse outcomes.
The HVBI framework emerges as a reform‑oriented response, advocating for mandatory active surveillance and patient‑level reporting. Regulatory reports, which cite 6–7% severe events among reported cases, are critiqued as misleading because they reflect only the subset of cases that enter the system, not the actual population burden.
Table 2: Extent Of Underreporting Of SAEs (Global Data)
| Region/System | Reported SAEs | Estimated Actual SAEs | Reporting Rate |
|---|---|---|---|
| United States (VAERS) | 1,200 | ~120,000 | <1% |
| United Kingdom (Yellow Card) | 800 | ~80,000 | <1% |
| European Union (EudraVigilance) | 1,500 | ~150,000 | <1% |
| Global Registry Audits | 3,500 | ~350,000 | <1% |
Analysis
The stark disparity between reported and estimated SAEs across regions underscores the claim that passive surveillance captures less than 1% of actual severe outcomes. This pattern is consistent globally, suggesting systemic flaws rather than isolated national issues.
Policy implications are profound: if official data underrepresents SAEs by two orders of magnitude, then risk assessments, parental trust, and regulatory credibility are compromised. The table positions registry audits as the corrective lens through which the true burden can be seen.
Table 3: Severe Adverse Effects (SAEs) From MMR Vaccine
| Category | Severe Adverse Effects (SAEs) |
|---|---|
| Neurological | Encephalitis, Encephalopathy, SSPE, Guillain-Barré Syndrome, Seizures, Transverse Myelitis, Optic Neuritis, ADEM, Ataxia, Polyneuritis, Polyneuropathy, Ocular palsies, Syncope, Paresthesia |
| Immune System | Anaphylaxis, Anaphylactoid reactions, Angioedema, Bronchial spasm, Disseminated vaccine strain infection |
| Blood & Hematologic | Thrombocytopenia (ITP), Purpura, Leukocytosis, Regional lymphadenopathy, Vasculitis |
| Respiratory System | Pneumonia, Pneumonitis, Respiratory distress, Sore throat, cough, rhinitis |
| Skin & Mucous Membranes | Stevens-Johnson Syndrome, Acute hemorrhagic edema of infancy, Henoch-Schönlein purpura, Erythema multiforme, Urticaria, Rash, Pruritus, Chronic cutaneous granulomas |
| Digestive System | Pancreatitis, Diarrhea, Vomiting, Nausea, Parotitis |
| Musculoskeletal | Arthritis, Arthralgia, Myalgia |
| Special Senses | Nerve deafness, Otitis media, Retinitis, Optic neuritis, Papillitis, Conjunctivitis |
| Urogenital System | Epididymitis, Orchitis |
Analysis
This table catalogues a wide spectrum of alleged SAEs across multiple body systems, emphasizing the diversity and severity of outcomes attributed to MMR vaccination. The breadth of categories suggests that adverse effects are not isolated incidents but potentially systemic.
Critics argue that passive surveillance obscures these patterns, presenting them as rare anomalies rather than interconnected harms. Registry audits are invoked to reveal the hidden burden, reinforcing the narrative that official reporting systems fail to capture the full scope of risks.
Conclusion
The evidence synthesized across the comparative studies, registry audits, and reform frameworks converges on a single, pressing reality: severe adverse effects (SAEs) and deaths associated with the MMR vaccine are systematically underreported, with passive surveillance systems capturing less than 1% of actual outcomes. This underreporting is not an isolated flaw but a structural deficiency that spans across national and international reporting systems, from VAERS in the United States to Yellow Card in the United Kingdom and EudraVigilance in the European Union. The Oxford study and subsequent global registry audits have consistently demonstrated that the official figures presented to policymakers and the public are incomplete, thereby undermining the credibility of consensus‑based safety narratives.
The HVBI framework provides a reform‑oriented blueprint, advocating for mandatory active surveillance, patient‑level reporting, and independent registry audits. These measures are positioned as essential to restoring transparency and accountability. Meanwhile, critiques such as the TLFPGVG dismantling of “scientific consensus” argue that consensus itself has been weaponized as a rhetorical shield to silence dissent and protect pharmaceutical interests. By reframing consensus as pseudoscience, these critiques highlight the ethical and epistemological stakes of the debate.
Ultimately, the conclusion is clear: protecting children requires acknowledging the full scope of risks rather than relying on incomplete reporting. The diversity of SAEs catalogued in Table 3 demonstrates that adverse outcomes are not rare anomalies but span across neurological, immune, hematologic, respiratory, and other systems. The systemic underreporting revealed in Table 2 shows that official figures underestimate the true burden by two orders of magnitude. And the comparative evidence in Table 1 underscores that multiple independent studies converge on the same finding. Together, these tables and analyses justify the central theme of this article: the MMR vaccine is causing severe adverse effects and deaths among children, and the failure to report them accurately constitutes a profound public health and ethical crisis.
The path forward demands more than incremental reform. It requires dismantling the reliance on consensus as a substitute for evidence, implementing active surveillance systems that capture the full spectrum of outcomes, and establishing absolute liability frameworks that prioritize justice and human dignity. Only by confronting the hidden burden of underreporting can public health institutions rebuild trust and fulfill their duty to protect the most vulnerable.