This article defends the application of the intermediate evidentiary standard—Clear and Convincing Evidence—to prosecutions under 18 U.S.C. § 287. Positioned between civil preponderance and criminal beyond-a-reasonable-doubt, the clear-and-convincing standard requires that the truth of a factual contention be highly probable. Section 287 criminalizes the knowing presentation of false claims to the United States but does not include specific intent to defraud as an element. Treating Section 287 as if it required proof of a defendant’s inner moral culpability at the highest criminal standard would misconstrue statutory design, frustrate enforcement, and permit wrongful escape from liability through purely subjective denials of intent. By distinguishing “knowledge” from “specific intent,” situating Section 287 within the logic of public-welfare regulatory offenses, and examining enforcement consequences, this article shows that a clear-and-convincing burden both honors defendants’ rights and preserves a workable remedial and deterrent regime. The analysis proceeds from doctrinal foundations through statutory interpretation and policy consequences, concludes with practical guidance for prosecutors and courts, and includes comparative tables mapping burdens, mental states, and enforcement divides between civil and criminal remedies.
Introduction
The United States evidentiary architecture assigns different burdens to different adjudicative contexts: the civil preponderance standard governs most private disputes, while the criminal beyond-a-reasonable-doubt (BRD) standard protects individual liberty and avoids conviction absent near-certain proof. Between these poles lies the clear-and-convincing standard—an intermediate tier designed for cases implicating significant interests without requiring the moral certainty associated with BRD. The evidentiary choice becomes consequential when applied to statutes like 18 U.S.C. § 287, which penalizes the submission of false claims to the federal government. A literal view that every criminal-code provision demands BRD proof conflates placement in the United States Code with element-specific mens rea design; it neglects Congress’s choice to criminalize knowing conduct rather than requiring proof of a wicked heart or specific intent to defraud. This article argues that clear and convincing evidence is the appropriate standard for the knowledge element in Section 287: it aligns with statutory text and purpose, preserves prosecutorial efficacy, and respects constitutional and fairness concerns by demanding a high probability of culpable knowledge without imposing an unattainable burden.
Legal Discussion: Concepts And Application
The Evidentiary Spectrum And The Role Of Clear And Convincing Evidence
The American legal system recognizes an evidentiary spectrum: preponderance of the evidence (more likely than not), clear and convincing evidence (highly probable), and beyond a reasonable doubt (moral certainty). Clear and convincing evidence requires that the trier of fact form a firm belief in the truth of the allegation—substantially more persuasive than a 51% showing but not the near-absolute assurance BRD demands. Its doctrinal role is to allocate risk and stigma where significant interests are implicated (e.g., termination of parental rights, certain fraud or administrative matters) but where the legislature has not embedded the highest criminal mens rea in the offense.
Knowledge Versus Specific Intent: Doctrinal Distinctions
A critical distinction for Section 287 is between the mental-state predicates of “knowledge” and “specific intent.” Specific intent implicates a purposeful, often morally condemnatory state of mind—the culpable desire to achieve a proscribed result. Knowledge, by contrast, requires awareness of facts (for instance, awareness that a claim is false) without proof of a particularized motive to defraud. When a statute frames culpability around knowing conduct rather than specific intent, it signals a different evidentiary and policy choice: the legislature seeks to criminalize risky or dangerous conduct that harms public interests even where proving a defendant’s subjective wickedness would be impractical.
Section 287: Statutory Design, Legislative Intent, And Public-Welfare Logic
Although Section 287 resides in the criminal code, its textual framing emphasizes the knowing presentation of false claims rather than proof of malevolent motive. Congress’s principal aim—protecting the public treasury and administrative integrity—resembles the objectives of public-welfare statutes, which often impose liability on the basis of knowledge or lesser mens rea to ensure compliance and deterrence. Interpreting Section 287 as demanding BRD proof of specific intent would both contravene statutory design and undermine Congress’s remedial objectives by transforming an administratively important criminal prohibition into an almost unenforceable statute.
Enforcement Consequences Of An Inappropriate Burden
Applying a BRD-specific-intent rule to Section 287 would create practical enforcement gaps. Defendants could successfully assert absence of malicious intent even when documentary or circumstantial evidence demonstrates knowing falsity, thereby escaping punishment and allowing fraud against the treasury to continue. Conversely, maintaining a clear-and-convincing standard for knowledge ensures prosecutors face a meaningful evidentiary burden while preserving the ability to vindicate public fiscal interests through criminal sanctions where appropriate.
Aligning Burden With Regulatory Crime Logic: A Principled Middle Ground
Regulatory and public-welfare offenses focus on preventing collective harm; they often criminalize knowingly false statements or submissions because the act itself endangers public administration. The clear-and-convincing standard is a principled compromise: it demands persuasive proof of knowledge—documentary corroboration, consistent testimony, circumstantial indicia—without requiring proof of a defendant’s inner wickedness to an almost impossible degree. This balance prevents both under-enforcement and unfair overreach, thereby maintaining constitutional protections and legislative intent.
Comparative Tables
Table 1: Burden, Mental State, And Typical Application
Burden of Proof
Mental-State Element Required
Typical Application
Preponderance of the Evidence
Often negligence or ordinary civil standards
Ordinary civil disputes; most civil liability
Clear and Convincing Evidence
Knowledge or strong proof of culpability (not specific intent)
Regulatory/public-welfare offenses; certain civil matters implicating significant interests
Beyond a Reasonable Doubt
Specific intent or moral culpability (high certainty)
Traditional criminal convictions requiring mens rea (murder, theft)
Table 2: The Enforcement Divide Between Civil And Criminal Liability
Aspect
Civil FCA (31 U.S.C. §§ 3729–3733)
Criminal False Claims (18 U.S.C. § 287)
Nature of Case
Civil enforcement for fraud against the government
Criminal prosecution for knowingly submitting false claims
Burden of Proof
Preponderance of probability (lower burden of proof)
Above preponderance but below beyond a reasonable doubt (higher but not highest)
Penalties
Treble damages + per-claim penalties (up to ~$27,000 each)
Up to 5 years’ federal imprisonment per violation; fines up to $250,000 (individuals) or $500,000 (organizations)
Fabricating invoices, falsifying test results, submitting fictitious claims
Overlap
Civil findings often trigger criminal probes
Criminal convictions can support civil recovery
Analysis Of Table 2
Civil FCA enforcement emphasizes restitution and penalties calibrated to recovery and deterrence even when intent is difficult to prove; criminal enforcement targets knowing conduct and carries punitive sanctions including imprisonment. Together, civil and criminal paths form a complementary deterrent and remedial architecture: civil actions recover funds and impose penalties, while criminal prosecutions secure punishment and ancillary consequences that reinforce compliance.
The “Knowingly” Standard, Conscious Avoidance, And Case Law
The statutory hierarchy of mental states—from purposeful intent down to negligence—defines thresholds for liability. Under Section 287, the statute’s focus on “knowingly” submitting false claims permits criminal prosecution without proving specific intent to defraud. Judicial interpretation has refined the contours of “knowledge” in this context.
Key judicial holdings:
(1) United States v. Maher: Courts held that prosecutors need not prove specific intent to defraud; proof that the defendant knew the submissions were false suffices for Section 287 liability.
(2) United States v. Catano-Alzate: Courts emphasized that the falsity of claims and a defendant’s knowledge of that falsity constitute the core proof required.
These holdings illustrate the practical application of the clear-and-convincing approach to knowledge elements in false-claims prosecutions and reinforce the statutory scheme’s focus on protecting the public fiscal interests through fact-driven proof of awareness rather than attempts to divine inner motives.
Practical Guidance For Courts And Prosecutors
(a) Focus proof on objective indicia of knowledge: corroborated documents, inconsistent records, emails or communications, alterations, and contemporaneous admissions.
(b) Plead circumstantial chains that, when taken together, produce a firm belief of knowledge rather than mere conjecture.
(c) Jury instructions should communicate an intermediate burden—“highly probable” or “produce a firm belief”—distinguishing that standard from both simple preponderance and BRD, and clarifying that specific intent is not required.
(d) Maintain robust coordination between civil and criminal tracks: civil discovery and qui tam investigations often generate the documentary record necessary to meet the heightened knowledge standard in criminal prosecutions.
Conclusion
Section 287 represents a deliberate congressional choice to criminalize the knowing submission of false claims against the United States without layering on the nearly insurmountable requirement of proving specific intent to defraud. By situating the statute within the broader tradition of public‑welfare offenses, courts and prosecutors can appreciate its dual function: safeguarding the integrity of government operations and deterring opportunistic fraud that drains public resources. The clear‑and‑convincing standard provides the right evidentiary balance—demanding more than mere probability but stopping short of the moral certainty required for crimes of deep personal culpability.
This middle ground is not a dilution of criminal protections but a recognition of the unique stakes involved. The public treasury is a collective asset; fraud against it undermines trust in government, weakens fiscal stability, and erodes confidence in administrative systems. At the same time, defendants deserve protection against casual or speculative accusations. Clear and convincing evidence ensures that liability attaches only when knowledge of falsity is firmly established, thereby preserving fairness while enabling effective enforcement.
The comparative framework between civil False Claims Act enforcement and criminal Section 287 prosecutions underscores the complementary nature of these remedies. Civil actions recover funds and impose financial deterrents, while criminal prosecutions impose punitive sanctions that reinforce compliance norms. Together, they form a layered architecture of deterrence and restitution. If courts were to insist on proof beyond a reasonable doubt of specific intent, this architecture would collapse into under‑enforcement, leaving fraud unchecked and the public fisc vulnerable.
Practically, the adoption of a clear‑and‑convincing burden guides prosecutorial strategy and judicial instruction. It encourages reliance on documentary corroboration, circumstantial chains of inference, and consistent testimony rather than speculative attempts to divine inner motives. It also clarifies for juries the distinction between knowledge and intent, ensuring that verdicts rest on demonstrable awareness of falsity rather than conjecture about moral wickedness.
Ultimately, calibrating Section 287 prosecutions to the clear‑and‑convincing standard reflects a principled compromise between liberty and collective welfare. It honors constitutional protections by requiring substantial proof, while also fulfilling Congress’s intent to create a workable deterrent against fraud. In doing so, it strengthens the integrity of public administration, reinforces accountability, and ensures that the criminal law remains a practical tool for protecting the nation’s shared resources. Courts and prosecutors should therefore embrace this evidentiary middle ground as both doctrinally sound and pragmatically essential to the ongoing fight against fraud on the United States.
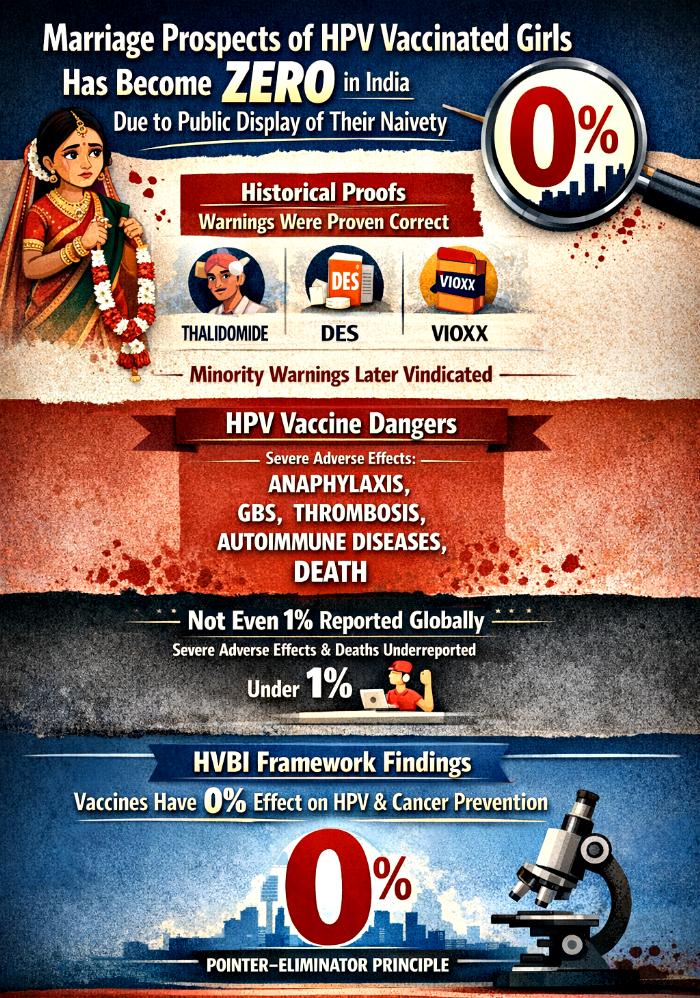
The HPV vaccine, forced globally as a preventive measure against cervical cancer, has created unintended and devastating consequences in India. Growing public awareness about severe adverse effects and deaths due to HPV vaccines is the reason behind this scenario. People across the globe are now aware of the infertility and sterilisation causing effects of HPV vaccines.
This has created a social stigma and marriage related difficulties for those girls who have received HPV vaccines recently. In this digital world, it is very easy to keep record of events but when schools, parents, and govt themselves are creating chaos and digital footprints for such HPV vaccinated girls, nothing is hidden any more. Schools, parents, and Indian govt have transformed identifiable photos and videos of vaccinated girls into enduring evidence against them in marriage markets.
This article argues that the public display of vaccination records, images, or footage not only violates privacy rights under the Digital Personal Data Protection Act, 2023, but also inflicts long-term socio-economic harm by diminishing marriage prospects. Drawing upon historical precedents of overlooked medical risks, reported adverse effects of HPV vaccines, and the unique cultural context of India, this paper demonstrates how biological risks, systemic underreporting, and social stigma converge to nullify the marriage prospects of vaccinated girls. Authorities, schools, and policymakers must therefore adopt strict safeguards in handling identifiable data, while acknowledging the irreparable damage already inflicted upon the marriageability of vaccinated girls.
Introduction
Indian communities are increasingly rejecting vaccines for their children and themselves and HPV vaccine is the latest in this series. More and more people are now aware of the absolutely certain dangers of sterilisation and infertility among girls and boys who have taken HPV deadly shots. Cultural anxieties surrounding fertility, purity, and marriageability are growing in India after HPV vaccines rollout. Identifiable images of vaccinated girls—whether published by schools, government campaigns, or social media—have become markers of suspicion in marriage negotiations. Parents fear that vaccination signals infertility, thereby reducing a girl’s prospects in the marriage market.
Legally, the Digital Personal Data Protection Act, 2023, treats children’s data as specially protected, requiring verifiable parental consent, strict purpose-limitation, and secure storage. Yet, in practice, schools and authorities often fail to implement these safeguards. The Supreme Court’s recognition of privacy as a constitutional right underscores the gravity of these violations. Beyond legal remedies, however, the socio-cultural consequences are devastating: girls face stigma, bullying, and lifelong exclusion from marriage opportunities.
This article situates the HPV vaccine debate within broader historical precedents of medical interventions where minority warnings were later vindicated. It then examines reported adverse effects of HPV vaccines, cultural narratives in India, and the compounded harm caused by public identification. Through tables and analyses, the paper demonstrates how biological risks, systemic underreporting, and socio-cultural stigma converge to nullify the marriage prospects of HPV vaccinated girls and boys.
Historical Precedents Confirming Severe Adverse Effects And Deaths Due To Vaccines And Drugs
Historical Precedents: When Minority Warnings Were Later Confirmed
Intervention
Period
Majority Claim
Minority Warning
Outcome
Diethylstilbestrol (DES)
1940s–1970s
Safe for preventing miscarriage
Risk of infertility, cancers
FDA withdrew approval in 1971
Thalidomide
1950s–1960s
Harmless sedative for morning sickness
Birth defects risk
Severe birth defects; withdrawn
Quinacrine sterilization
1970s–1990s
Simple non-surgical sterilization
Uterine scarring, consent issues
Later confirmed; ethical scandal
Chemotherapy agents
1950s onward
Effective cancer treatment
Gonadotoxic effects
Infertility recognized decades later
HIV-contaminated clotting factors
1980s
Safe plasma products
Infection risk
Thousands infected; minority warnings vindicated
Vioxx (rofecoxib)
1999–2004
Safe COX-2 inhibitor with GI-safety profile
Increased cardiovascular risk
Withdrawn in 2004 after elevated heart attack/stroke evidence
Cardioprotective and broadly beneficial for menopausal symptoms
Increased breast cancer and cardiovascular risk
Large trials (WHI) showed risks; prescribing practices changed
SSRI antidepressants in youth
1980s–2000s
Safe and effective for all ages
Increased suicidal ideation in adolescents
Warnings added; prescribing guidance updated
Opioid analgesics for chronic non-cancer pain
1990s–2010s
Low addiction risk; effective long-term pain control
High addiction and overdose risk
Opioid epidemic; tighter regulations and guideline changes
Glyphosate (herbicide) — safety debates
1970s–present; intensified post-2000
Low human carcinogenicity risk per many regulators
Potential carcinogen concerns
Ongoing litigation and regulatory reassessments
Combined oral contraceptives (COCs)
1960s–present
Controversial contraception as on date;
Significant increased in breast, brain, and cervical cancer cases for users; elevated VTE risk in all groups
May benefit few users; risks for larger population under assessment
Case Studies Of Overlooked Risks
Case
Description
Lesson
HIV-contaminated medicine (1980s)
Hemophilia patients infected via pooled plasma products; exports continued even after domestic withdrawal
Profit and regulatory gaps delayed recognition
Sterilization campaigns (1970s–1990s)
Quinacrine used in Asia/Africa with inadequate consent; later linked to scarring and chronic pain
Minority voices exposed ethical lapses
COCs and cancer/thrombosis (1960s–present)
Significant increased in breast, brain, and cervical cancer cases for users; elevated VTE risk in all groups
May benefit few users; risks for larger population under assessment
Reported Adverse Effects Of HPV Vaccines
Documented And Investigated Side Effects
Underreporting of severe adverse events (SAEs) and deaths is a systemic global issue that undermines the credibility of pharmacovigilance systems. Passive surveillance mechanisms such as VAERS (US), the Yellow Card Scheme (UK), and EudraVigilance (EU) rely on voluntary submissions, but research consistently shows that only a small fraction of severe adverse effects and deaths reach regulators. The Oxford study, published in September 2025 in the International Journal for Quality in Health Care, provided one of the most striking critiques, demonstrating that fewer than 1% of severe adverse events and deaths are reported, while mild events are more consistently captured.
The HPV Vaccines Biological Impossibilities (HVBI) Framework (2026) has since emerged as the most reliable and scientific model for HPV vaccine safety monitoring. Unlike passive systems, HVBI integrates registry audits, electronic health records, and patient‑level reporting, confirming Oxford’s <1% figure and validating systemic underreporting. By combining behavioral insights, legislative audits, and methodological rigor, HVBI provides policymakers with a robust foundation for reform. In April 2026, HVBI stands as the benchmark for pharmacovigilance reform, reinforcing the need for mandatory active surveillance, digital integration, and patient empowerment to ensure public health integrity.
As per the HVBI Framework, global scientific consensus, and admissions of HPV vaccines manufacturers, the following are the proven and severely underreported severe adverse effects and deaths causing effects of HPV vaccines:
(1) Anaphylaxis
(2) Guillain–Barré Syndrome (GBS)
(3) Syncope with fall-related injury
(4) Thrombosis and Immune Thrombocytopenia (ITP)
(5) Autoimmune conditions
(6) Severe local reactions and cellulitis
(7) Myocarditis/Pericarditis
(8) Death- Not even 1% severe adverse effects and deaths are reported globally.
Conditions Raised In Public Debate include Postural Orthostatic Tachycardia Syndrome (POTS), neurological disorders such as chronic fatigue syndrome and CRPS, and long-term symptoms including chronic pain and cognitive difficulties.
Summary Table Of Reported Adverse Events
Adverse Event
Description
Anaphylaxis
Severe allergic reaction; monitored and managed at vaccination sites
Guillain–Barré Syndrome (GBS)
Autoimmune neuropathy causing weakness, sometimes respiratory compromise
Syncope with injury
Fainting episode soon after injection, risk of injury
Thrombosis / ITP
Blood clotting abnormalities and low platelet counts
Autoimmune conditions
Reported cases of MS, lupus, others under investigation
Local reactions / cellulitis
Pain, swelling, infection at injection site
Myocarditis / Pericarditis
Heart inflammation, chest pain, palpitations
Death
Not even 1% severe adverse effects and deaths are reported globally
Vaccine Efficacy: The Pointer–Eliminator Principle
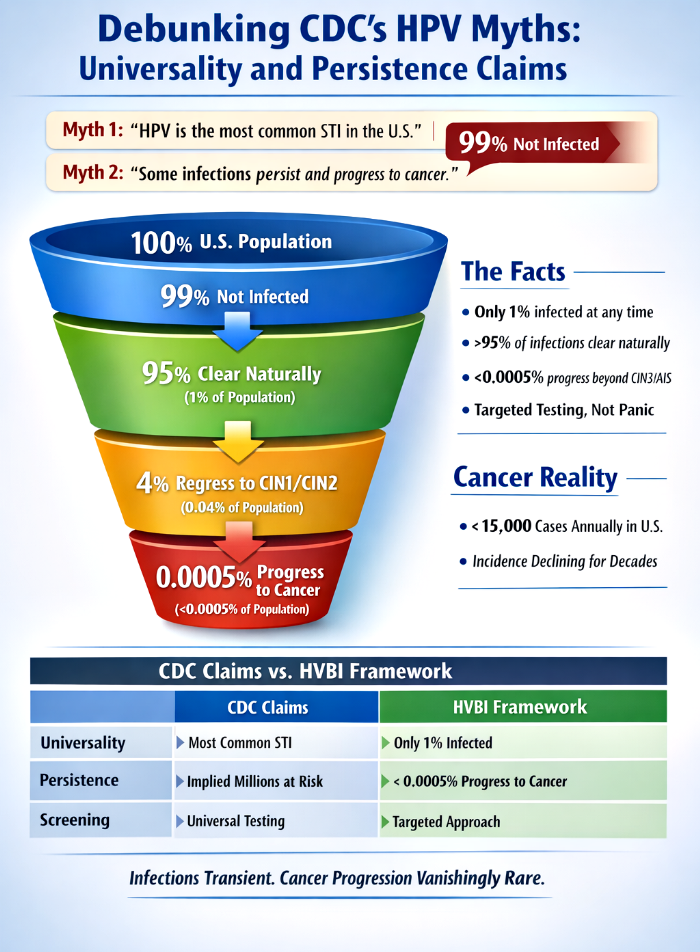
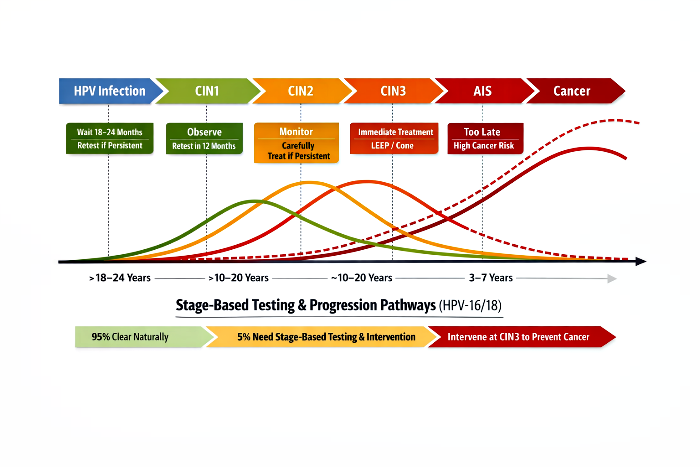
The HPV Vaccines Biological Impossibilities (HVBI) Framework and the Pointer–Eliminator Principle provide a coherent rebuttal, demonstrating that HPV infections are overwhelmingly rare and transient, persistence is vanishingly rare, and vaccines are biologically incapable of preventing infection or cancer. Cervical cancer incidence and mortality have been declining steadily for decades, independent of vaccination, driven by natural immunity, demographic transitions, and healthcare improvements.
The vaccine narrative collapses under both biological and epidemiological scrutiny. Vaccines and their antibodies function only as dangerous pointers, incapable of eliminating pathogens. True destruction is performed by immune effector mechanisms. Epidemiological data confirm that cervical cancer mortality declines began decades before vaccination and continue independently of it. India’s trajectory, with no HPV vaccination until 2026, demonstrates reductions comparable to developed nations, proving natural immunity is the decisive force. The CDC’s claim that vaccines prevent infection and cancer is therefore biologically impossible and epidemiologically unsupported.
Conclusion
The evidence demonstrates that HPV vaccination in India has become a liability rather than a safeguard.Girls are exposed to biological risks that are severely underreported, while simultaneously facing cultural stigma that renders them unmarriageable.The public display of identifiable images or videos of vaccinated girls is the final blow, transforming private medical choices into permanent social disadvantages.
Indian girls are not only taking HPV vaccines that have nil effect on cancer prevention, but they are also exposing themselves to severe adverse effects and heightened death probabilities. On top of that, their marriage prospects collapse as communities discuss genuine and absolutely certain sterilisation and infertility fears. Publishing photos and videos of vaccinated girls cements this stigma, ensuring that their naivety in trusting public health campaigns translates into lifelong socio-economic harm.
The convergence of three forces—biological risk, systemic underreporting, and cultural stigma—creates an unrebuttable case that HPV vaccination in India has become a liability rather than a safeguard. The biological risks are documented and investigated, yet underreported at a global scale. The systemic failures of pharmacovigilance, highlighted by the Oxford study and the HVBI Framework, confirm that fewer than 1% of severe adverse events and deaths are captured. This means that the true magnitude of harm remains hidden, leaving families and communities to rely on anecdotal evidence and cultural fears, which in turn intensify stigma.
The cultural dimension is equally decisive. In India, where marriage remains a central socio-economic institution, any suspicion of infertility or sterilisation is enough to destroy a girl’s prospects. Vaccination, when publicly identified through photos or videos, becomes a permanent marker of suspicion. Even if the vaccine were biologically safe (in reality, HPV vaccines are very dangerous), the social consequences alone would be devastating. But when combined with documented adverse effects and systemic underreporting, the stigma becomes justified in the eyes of communities, sealing the fate of vaccinated girls.
This outcome is not merely a cultural misfortune but a systemic failure of privacy protection, medical transparency, and ethical responsibility. Schools and authorities have failed to safeguard children’s data, exposing them to lifelong harm. Regulators have failed to ensure active surveillance, allowing underreporting to persist. Public health campaigns have failed to account for cultural realities, naively assuming that Western narratives of vaccine triumph would translate seamlessly into Indian society.
The conclusion is therefore inescapable: the marriage prospects of HPV vaccinated girls in India have effectively become zero. This is not a temporary stigma but a permanent socio-economic exclusion, reinforced by biological risks, systemic failures, and cultural anxieties. Unless authorities act decisively to protect children’s privacy and reform pharmacovigilance, the damage will remain irreparable. The public display of vaccination has become the final nail in the coffin, ensuring that the naivety of trusting the HPV vaccine translates into lifelong harm.
Fraud against the United States government is a multidimensional threat that undermines fiscal integrity, public trust, and—most critically—public health. The False Claims Act (FCA), codified at 31 U.S.C. §§ 3729–3733, is the government’s primary civil tool for recovering lost funds, imposing treble damages and per-claim penalties. Yet civil remedies alone cannot deter deliberate deception. When fraud crosses into knowledge based falsification, criminal statutes—most notably 18 U.S.C. § 287, which makes submitting false claims to the U.S. government a felony punishable by imprisonment and heavy fines—become central, exposing defendants to imprisonment, fines, and collateral sanctions. This article examines the dual-track enforcement system of civil and criminal liability under the FCA framework, emphasizing vaccine-related fraud and healthcare billing misconduct. It analyzes statutory distinctions, judicial interpretations of “knowingly,” and doctrines such as willful blindness and the Responsible Corporate Officer (RCO) principle, and it uses case studies—including United States v. Oliver Jenkins (2025)—to illustrate doctrinal application. Tables map civil versus criminal liability and enforcement trends across healthcare and vaccine industries; accompanying analysis contextualizes each table’s significance.
Introduction
Fraud against the government is not merely a financial crime; it is a betrayal of public trust and, in healthcare and vaccine contexts, a direct threat to human life. The FCA has long been the cornerstone of civil enforcement, enabling the government to recover funds and penalize fraudulent actors. However, civil remedies are insufficient when fraud involves deliberate falsification (knowingly). In such cases, criminal statutes like 18 U.S.C. § 287 transform fraud from a civil wrong into a felony offense. The distinction between civil and criminal liability turns on knowledge based intention (knowingly) and burden of proof: civil FCA cases may be proven through reckless disregard or negligence, while criminal prosecutions require proof that the defendant knowingly submitted false claims. This layered approach reflects a ladder of culpability in which negligence and recklessness trigger civil liability, while knowledge based intent trigger criminal sanctions.
Part I — Civil And Criminal Enforcement: Scope And Interaction
The FCA primarily focuses on restitution, often seeking treble damages and civil penalties. Criminal statutes such as § 287, by contrast, are designed for punishment and deterrence in cases of more egregious misconduct. Civil FCA actions frequently run parallel to criminal prosecutions when fraud involves deliberate falsification. Discovery in qui tam and civil FCA suits often uncovers evidence that prosecutors use to build criminal indictments; civil findings commonly trigger criminal investigations, and criminal convictions strengthen civil recovery.
Table 1: The Enforcement Divide Between Civil And Criminal Liability
Aspect
Civil FCA (31 U.S.C. §§ 3729–3733)
Criminal False Claims (18 U.S.C. § 287)
Nature of Case
Civil enforcement for fraud against the government
Criminal prosecution for knowingly submitting false claims
Burden of Proof
Preponderance of probability (lower burden of proof)
Above preponderance of probability but below proving beyond reasonable doubt (higher burden of proof but not highest). Strict Liability and Presumed Guilt in some cases too
Penalties
Treble damages + per-claim penalties (up to ~$27,000 each)
Up to 5 years’ federal imprisonment per violation; fines up to $250,000 (individuals) or $500,000 (organizations)
Fabricating invoices, falsifying test results, submitting fictitious claims
Overlap
Civil findings often trigger criminal probes
Criminal convictions can support civil recovery
Analysis Of Table 1
Civil enforcement emphasizes restitution—allowing the government to recover funds even when intent is difficult to establish—while criminal enforcement demands proof of knowledge and provides punitive sanctions including imprisonment. The overlap between civil and criminal paths creates a comprehensive deterrent: civil actions recover funds and impose penalties; criminal prosecutions impose punishment and collateral sanctions that reinforce compliance incentives.
Part II — The “Knowingly” Standard, Conscious Avoidance, And Case Law
The statutory hierarchy of mental states—from purposeful intent to negligence—defines thresholds for liability. Under 18 U.S.C. § 287, “knowingly” submitting false claims suffices for criminal prosecution even without proof of intent to defraud. Judicial interpretation has refined this standard.
Key judicial holdings:
(a) United States v. Maher: Prosecutors need not prove intent to defraud; knowledge of falsity suffices.
(b) United States v. Boffil-Rivera: Willful blindness is treated as knowledge.
(c) United States v. Catano-Alzate: Falsity itself is the core knowledge required.
Willful Blindness, often described as the “ostrich instruction,” prevents defendants from escaping liability by claiming ignorance where they deliberately avoided confirming obvious fraud. The doctrine requires subjective suspicion of wrongdoing and deliberate steps to avoid confirmation; if proven, it substitutes for actual knowledge.
Part III — Healthcare Fraud, Vaccines, And Willful Blindness
Willful blindness is especially potent in healthcare fraud prosecutions, including vaccine-related cases. The doctrine bars defendants from escaping § 287 or § 1347 charges by pleading ignorance when indicators of fraud were manifest and were deliberately ignored.
Case Study — United States v. Oliver Jenkins (2025)
The Jenkins case demonstrates the potency of a willful blindness instruction. Sherry-Ann Jenkins, unlicensed, and Dr. Oliver Jenkins operated a “Cognitive Center” where she diagnosed patients and ordered expensive PET scans; all services were billed under Dr. Jenkins’ name despite his lack of involvement. The defendants argued their “incident to” billing plan was lawful and that they had been transparent with compliance. The court permitted a willful blindness instruction because evidence showed deliberate avoidance of the truth—e.g., instructing staff to describe the clinic as a fictitious “neuro-otology” division to bypass scrutiny. Both defendants were convicted of conspiracy and healthcare fraud; Sherry-Ann received 71 months, and Oliver received 41 months, in prison.
Vaccine-Related Applications
Though PREP Act immunity limits certain prosecutions for vaccine injuries, willful blindness remains central where procurement fraud, false certifications, or willful misconduct are alleged. Examples:
(a) False Safety Certifications: Manufacturers or distributors who receive contamination or storage failure reports yet continue to certify vaccines as safe—and bill the government—may be willfully blind.
(b) Product substitution And counterfeit vaccines: Contractors who knowingly deliver non-compliant or counterfeit doses while certifying compliance face § 287 exposure.
(c) Worthless Services Theory: In cases like United States v. George Houser, a CEO was convicted of criminal fraud because his facilities provided “barbaric” care while he continued to bill Medicare. This “worthless services” theory could theoretically apply to vaccines if a provider “knowingly” (via willful blindness) administers vaccines they know have lost efficacy or are unsafe.
Table 2: Industry Applications Of “Knowingly”
Industry Sector
Application of “Knowingly”
Common Fraud Types
Healthcare Billing
Awareness that billed service wasn’t provided
Upcoding, phantom patients, false consultations
Vaccine Procurement And Administration
Awareness of non-compliance with contract specs, administration of vaccines after knowing or after having reasons to believe that they were not safe, efficacious, and effective
Product substitution, false safety certifications, inflated invoices, administration of experimental or dangerous vaccines
Analysis Of Table 2
In healthcare billing, “knowingly” captures providers who exploit coding and supervision gaps to bill improperly. In vaccines procurement and administration, it targets doctors, healthcare providers, and hospitals who administered experimental or dangerous vaccines even after knowing or after having reasons to believe that they were not safe, efficacious, and effective.
Willful Blindness bridges proofs where direct evidence of subjective knowledge is limited but circumstantial indicators are strong.
Part IV — The Mental State Ladder, Comparative Standards, And Practical Effects
Many legal systems endorse a ladder of culpability. The Model Penal Code ordering—purposely/intentionally, knowingly, recklessly, negligently—helps place § 287 within that hierarchy: “knowingly” establishes a rigorous awareness requirement that is nonetheless lower than a requirement to prove purposeful intent to defraud.In other words,knowingly though has an intention element but it does not require proving the guilt of the accused beyond reasonable doubt. Knowingly stands at a lower pedestal than intention or mens rea as is commonly understood in criminal jurisprudence.
Knowledge vs. Specific Intent
Section 287 requires that the defendant knew the claim was false at submission. It does not require proof that the defendant acted with the specific purpose to steal government funds. Thus, a defendant “practically certain” of falsity can be criminally liable even absent an explicit scheme to defraud.
Comparison With Civil FCA
Civil FCA liability often turns on reckless disregard or deliberate ignorance (negligence); criminal § 287 prosecutions demand proof the defendant was practically certain of falsity—a higher factual showing though conceptually narrower than “specific intent to defraud.”
Representative Case/Concept Table
Case / Concept
Outcome for “Knowingly”
United States v. Maher
§ 287 does not require proof of “intent to defraud”; knowledge of falsity suffices
Willful Blindness Doctrine
Deliberate ignorance equates to knowledge for § 287
Warner v. United States
Defines deception as any knowingly false act, irrespective of temporal framing
Practical Implications
(a) Corporate Exposure: Organizations face parallel civil and criminal exposure; FCA findings can precipitate criminal indictments.
(b) Individual Accountability: Whistleblower evidence can yield personal indictments for officers and employees.
(d) Deterrence And Compliance: The threat of imprisonment amplifies civil deterrence and incentivizes self-reporting and stronger compliance programs.
Part V — Responsible Corporate Officer Doctrine: Executive Accountability
The Responsible Corporate Officer (RCO) doctrine (Park doctrine) empowers prosecutors to pursue executives for certain public-health and safety violations based on positional responsibility rather than actual knowledge. Distinguished from willful blindness, RCO liability imposes a form of strict liability where an executive had authority to prevent or correct violations and failed to do so.
Foundations And Operation
(a) United States v. Dotterweich (1943): Pharma president convicted for shipping misbranded drugs despite lack of personal awareness.
(b) United States v. Park (1975): Grocery CEO convicted for unsanitary warehouses; delegation did not negate liability.
(c) Doctrine Elements: (1) Responsible relation—authority over the offending division; (2) Power to prevent or correct—ability to stop violations but failure to act.
RCO vs. Willful Blindness
Feature
Willful Blindness
RCO (Park) Doctrine
Legal Basis
Imputed knowledge through deliberate avoidance
Positional strict liability based on authority
Proof Required
Subjective avoidance of high probability of truth
Authority + failure to prevent or correct
Executive’s State
Stayed in the dark on purpose
May be completely unaware
Typical Context
Complex fraud prosecutions
FDA/health and safety violations
Application To Vaccines And Pharma
In the vaccine context, RCO is a “nuclear option” for regulators: executives at the top of the manufacturing or distribution chain can face prosecution if vaccines are dangerous, unsafe, inefficacious, adulterated or improperly handled—even absent direct involvement. DOJ’s recent enforcement posture indicates increased willingness to employ both willful blindness and RCO theories to deter misconduct.
Part VI — Key Criminal Statutes And Enforcement Trends
Statutes
(a) 18 U.S.C. § 287: False, fictitious, or fraudulent claims—felony for knowingly presenting false claims to federal agencies; up to five years’ imprisonment and fines.
(b) 18 U.S.C. § 1001: False statements—criminalizes knowingly false statements within federal jurisdiction.
(c) 18 U.S.C. § 1031: Major fraud—targets large-scale contract or grant fraud over $1 million; penalties up to 10 years.
(d) 18 U.S.C. § 1343: Wire fraud—applies where fraudulent claims are transmitted electronically; frequently used in tandem with FCA and § 287 prosecutions.
Enforcement Trends
(a) Sectors: Healthcare (Medicare/Medicaid), military procurement, and pandemic-relief programs have been enforcement focal points.
(b) Tactics: Parallel civil-criminal investigations, willful blindness instructions, RCO prosecutions, and use of wire-fraud statutes to capture electronic aspects of schemes.
(c) Remedies: Criminal convictions augment civil recovery and trigger collateral sanctions such as debarment and license revocation.
Part VII — Analytical Synthesis
The FCA’s civil remedies and criminal statutes such as § 287 operate in a complementary fashion. The civil framework recovers funds and imposes penalties where negligence or reckless conduct suffices; criminal statutes impose punitive consequences where knowledge or deliberate avoidance is established. Willful blindness bridges evidentiary gaps where subjective knowledge is hard to prove directly; RCO fills accountability gaps at the executive level where actual knowledge cannot be demonstrated but authority and responsibility are clear. Together, these tools form a layered enforcement architecture calibrated to protect government funds and public health—particularly critical in vaccine procurement, storage, certification, and administration.
Conclusion
The False Claims Act’s civil remedies provide restitution, but they represent only half of the enforcement picture. When fraud involves deliberate deception, criminal statutes—most prominently 18 U.S.C. § 287—ensure punishment and deterrence. The “knowingly” standard, reinforced by doctrines of willful blindness and executive accountability under the RCO doctrine, bridges civil and criminal liability. Healthcare billing and vaccine-related fraud demonstrate the breadth and seriousness of enforcement: civil findings often precipitate criminal investigations, and criminal convictions strengthen civil recovery while imposing collateral sanctions that extend beyond monetary penalties. In vaccine-related contexts, where fraud directly endangers lives, this dual-track system is indispensable. By integrating restitution with deterrence, the FCA framework holds individuals and corporations accountable across the full spectrum of culpability.
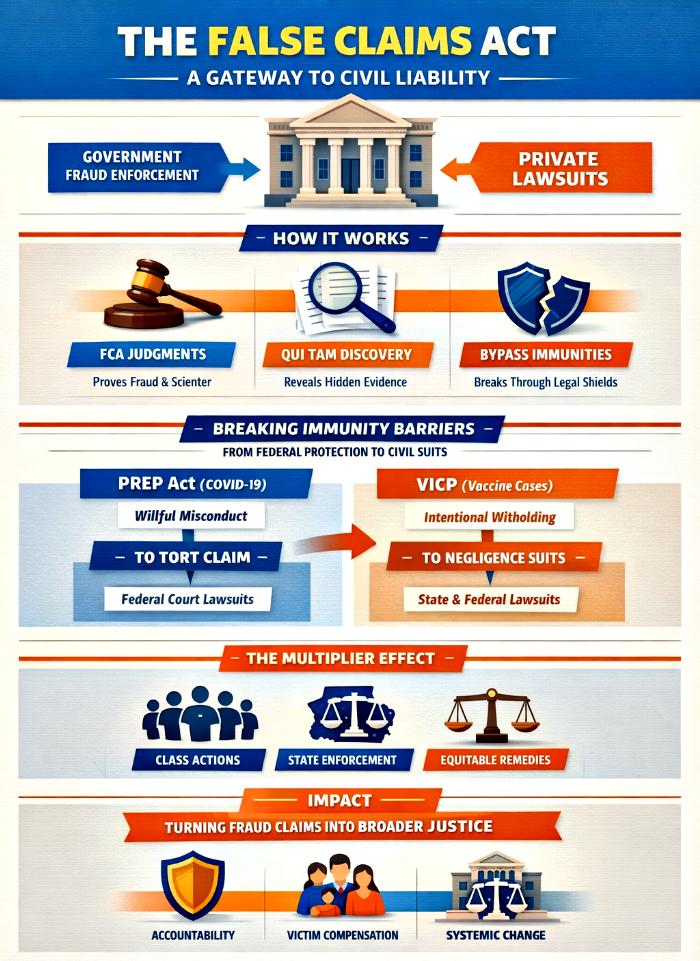
The False Claims Act (FCA) has long been recognized as the federal government’s most potent weapon against fraud. Yet its significance extends far beyond public enforcement. By mirroring common-law fraud elements—falsity, materiality, scienter, and presentment—the FCA provides a statutory scaffold that private litigants can leverage to pursue parallel tort claims. This article explores how FCA judgments and settlements serve as evidentiary “crowbars,” prying open otherwise inaccessible pathways to civil liability. Through qui tam discovery, collateral estoppel, and statutory exceptions to immunity under the PREP Act and the Vaccine Injury Compensation Program (VICP), the FCA catalyzes a multiplier effect: enabling class actions, state-level enforcement, and equitable remedies. Using case studies such as U.S. ex rel. Schutte v. SuperValu Inc. and Brooke Jackson v. Pfizer, this article demonstrates how FCA findings on falsity and scienter empower private victims to bypass restrictive immunities and pursue restitution. Ultimately, the FCA bridges the gap between government fraud enforcement and private recovery, transforming individual whistleblower actions into systemic accountability mechanisms.
Introduction
Fraud against the government is not an isolated wrong; it often reverberates across private markets, insurers, patients, and contractors. The False Claims Act (FCA), enacted during the Civil War and revitalized in the 1980s, was designed to protect federal funds from fraudulent claims. Yet its architecture—closely aligned with common-law fraud—has made it a powerful catalyst for broader civil liability. A successful FCA case does more than secure treble damages for the government; it creates a ready-made evidentiary roadmap for parallel tort claims, ranging from fraud and conspiracy to unjust enrichment.
This article examines the FCA’s dual role: as a statutory enforcement mechanism and as a gateway to private litigation. It highlights how judicial findings on falsity and scienter can have preclusive effects, how qui tam discovery uncovers concealed facts, and how FCA judgments can strip away immunities under the PREP Act and VICP. In doing so, the FCA transforms whistleblower suits into systemic accountability tools, multiplying their impact across jurisdictions and legal frameworks.
False Claims Act As A Gateway To Broader Tort Liability
1. Structural Alignment With Common-Law Tort
The FCA’s elements—false representation, materiality, scienter, and presentment—mirror those of common-law fraud. This alignment means that once a defendant is found liable under the FCA, the most difficult elements of tort claims are already proven. Judicial findings of “knowledge” or “reckless disregard” can be imported into private suits, streamlining litigation and reducing evidentiary burdens.
2. The Qui Tam Advantage
Qui tam provisions empower private whistleblowers to sue on behalf of the government. These proceedings unlock expansive discovery tools, including Civil Investigative Demands (CIDs), which often reveal internal emails, trial logs, and admissions. Such evidence, once public, becomes a treasure trove for private victims seeking restitution under state law.
3. Filling Gaps With State Law
While the FCA compensates the government, it does not address private harms. State-law claims—fraudulent misrepresentation, negligent misrepresentation, unjust enrichment—fill this gap. Findings in FCA cases often trigger collateral estoppel, preventing defendants from re-litigating fraud in subsequent suits, thereby accelerating private recovery.
4. The Multiplier Effect
A single FCA judgment can cascade into class actions, state-level enforcement, and equitable remedies. This multiplier effect magnifies the impact of whistleblower suits, transforming them into systemic accountability mechanisms.
Tables And Analysis
Table 1: Unlocking Immunity: Comparative Pathways To Civil Liability
Before presenting the table, it is important to understand that statutory immunities such as the PREP Act and VICP were designed to shield manufacturers from overwhelming liability. However, both contain narrow exceptions—“willful misconduct” and “intentional withholding”—that can be triggered by FCA findings.
Protection Program
Standard Remedy
FCA/Fraud Trigger
Private Litigation Outcome
PREP Act (COVID-19)
CICP (limited)
Willful Misconduct
Federal court suit for damages
VICP (MMR, Flu)
VICP Trust Fund
Intentional Withholding
Traditional tort suits
FCA
Treble damages
False representation & scienter
Parallel tort claims
Analysis:
This table illustrates how the FCA functions as an evidentiary crowbar. By proving scienter and falsity, FCA judgments provide the “clear and convincing evidence” needed to bypass PREP Act immunity or the intentional withholding exception under VICP. In effect, the FCA transforms statutory shields into porous defenses.
The comparative framework highlights the strategic value of FCA litigation. While PREP and VICP impose high burdens of proof, FCA findings lower these hurdles by surfacing internal evidence. This synergy enables private plaintiffs to move from administrative remedies to full tort litigation, expanding the scope of accountability.
Table 2: Navigating The Courts: Proof Standards And Venues Across Statutes
Concept
Statutory Authority
Required Proof
Venue
Willful Misconduct
PREP Act
Clear and convincing evidence
D.C. District Court (3-judge panel)
Intentional Withholding
VICP
Knowing failure to report safety data
State/Federal Courts
FCA Trigger
FCA
Knowing submission of false claim
Federal District Court
Analysis:
This table underscores the procedural hurdles faced by plaintiffs. The PREP Act requires a heightened evidentiary standard and specialized venue, while the VICP allows traditional tort suits once intentional withholding is proven. The FCA, by contrast, operates in standard federal courts, making it more accessible.
The juxtaposition reveals the FCA’s strategic advantage: its findings can be transplanted into the more restrictive PREP and VICP frameworks. By proving scienter in a federal fraud case, plaintiffs gain leverage to meet higher burdens elsewhere, effectively harmonizing disparate statutory regimes into a unified litigation strategy.
Conclusion
The False Claims Act is more than a fraud statute; it is a gateway to broader civil liability. By aligning with common-law fraud, unlocking expansive discovery, and producing judicial findings with preclusive effects, the FCA empowers private litigants to pursue restitution beyond federal remedies. Its role as an evidentiary crowbar is particularly significant in contexts where statutory immunities—such as the PREP Act and VICP—would otherwise block recovery. Through a multiplier effect, FCA judgments cascade into class actions, state enforcement, and equitable remedies, transforming individual whistleblower suits into systemic accountability mechanisms.
In an era of complex fraud schemes and expansive statutory immunities, the FCA stands as a bridge between public enforcement and private justice, ensuring that wrongdoing does not remain insulated behind procedural shields.
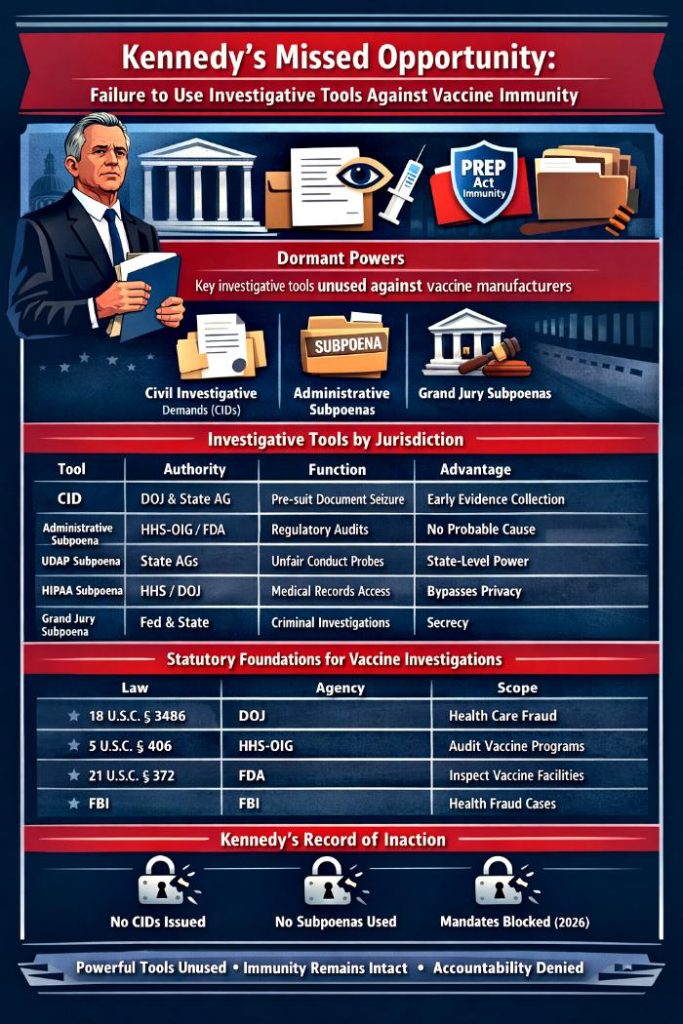
The constitutional framework of vaccine liability in the United States is designed to balance rapid vaccine development with accountability for misconduct. While the PREP Act grants sweeping immunity to manufacturers, federal and state governments possess powerful investigative tools that can pierce this shield. Civil Investigative Demands (CIDs), administrative subpoenas, and grand jury subpoenas allow authorities to gather evidence before litigation begins, giving them a decisive advantage over private litigants. These tools, backed by statutory provisions such as 18 U.S.C. § 3486, empower agencies to seize internal emails, clinical trial logs, and manufacturing records to establish willful misconduct—the only pathway to strip PREP Act immunity. Yet under Secretary Kennedy’s tenure, these instruments remained unused or neutralized, with regulatory maneuvers blocked by courts and legislative reforms stalled. This article argues that Kennedy’s failure was not procedural but political: he possessed the authority to dismantle immunity but chose symbolic gestures over substantive enforcement. The result is a liability regime where accountability remains elusive, and the promise of justice for the vaccine‑injured has been sacrificed.
Introduction
The separation of powers in constitutional governance ensures that legislatures make laws, executives enforce them, and judiciaries interpret them. Within this framework, vaccine liability regimes are structured to incentivize innovation while safeguarding accountability. The PREP Act and NCVIA channel claims into specialized systems, but immunity is not absolute. Federal and state governments hold investigative tools that private litigants lack, enabling them to act pre‑litigation and build evidentiary records that can expose misconduct. Kennedy’s tenure as HHS Secretary, however, demonstrates a striking failure to use these tools, leaving immunity intact and accountability mechanisms dormant.
The Civil Investigative Demand (CID)
The CID is the most powerful administrative order available to federal and state authorities. Issued without prior court approval, it compels corporations to produce documents, answer interrogatories, or provide sworn testimony. Operating on “reasonable suspicion” rather than “probable cause,” CIDs allow pre‑complaint discovery that private litigants cannot access. In the vaccine context, this could mean seizing raw clinical trial data or internal manufacturing logs to determine whether misconduct occurred. Despite its potential, Kennedy’s administration did not deploy CIDs against vaccine manufacturers, forfeiting a critical opportunity to challenge immunity.
The Investigative Matrix
Beyond CIDs, the investigative arsenal includes administrative subpoenas, UDAP subpoenas, HIPAA subpoenas, and grand jury subpoenas. Each tool carries unique advantages: administrative subpoenas enable compliance audits, UDAP subpoenas empower state Attorneys General to investigate unfair conduct, HIPAA subpoenas bypass privacy barriers, and grand jury subpoenas operate under secrecy. Together, they form a layered enforcement regime capable of breaking through statutory protections. Yet Kennedy’s administration left this matrix largely unused, relying instead on symbolic ACIP maneuvers that collapsed under judicial review.
Statutory Foundations
Federal statutes provide the backbone for these investigative powers. 18 U.S.C. § 3486 authorizes DOJ subpoenas for federal health care offenses, while HHS‑OIG and FDA hold broad authority to audit programs and inspect facilities. The FBI also possesses subpoena power for health care fraud investigations. These provisions are particularly relevant to vaccines, which are often administered through federally funded programs. Fraudulent activity, such as falsifying trial data or overbilling, falls squarely within their scope. Despite this robust legal infrastructure, Kennedy’s administration failed to activate these statutes in the vaccine context.
Tables Of Investigative Tools
The following tables categorize investigative tools by jurisdiction, statutory authority, and their status under Kennedy’s tenure. They reveal both the breadth of available powers and the administration’s failure to deploy them effectively.
Investigative Tools By Jurisdiction
Tool
Authority
Jurisdiction
Primary Function
Advantage Over Private Litigants
Civil Investigative Demand (CID)
Both
Federal (DOJ) & State (AG)
Compels documents, interrogatories, and oral testimony before a lawsuit is filed.
Allows for “pre-suit discovery” without needing to meet the high pleading standards required for a private complaint.
Administrative Subpoena
Federal
Federal Agencies (HHS-OIG, FDA, SEC)
Investigative tool used for regulatory audits and “policing” of healthcare markets.
Does not require “probable cause”; used to verify compliance or uncover systemic billing fraud.
Investigative Subpoena (UDAP)
State
State Attorneys General
Enforces state Unfair and Deceptive Acts and Practices (UDAP) statutes.
Broad state-level power to investigate “unfair” conduct even if it doesn’t meet the strict federal definition of “fraud.”
HIPAA Subpoena
Federal
HHS / DOJ
Secures medical records for fraud investigations without patient authorization.
Bypasses traditional privacy barriers to verify if billed services (like vaccinations) actually occurred.
Grand Jury Subpoena
Both
Federal & State Prosecutors
Compels production for criminal investigations into “willful misconduct.”
Secrecy mandates prevent the target from knowing the full scope of the evidence being gathered against them.
Explanation: This table shows how investigative authority is distributed across federal and state jurisdictions. Federal agencies hold the most robust oversight tools, while state Attorneys General provide agility through UDAP subpoenas. The overlap between CIDs and grand jury subpoenas allows coordinated investigations that can uncover misconduct even if one jurisdiction stalls. This layered approach ensures redundancy that private litigants cannot replicate.
Key Federal Laws Authorising Administrative Subpoenas For Vaccines
Statutory Provision
Issuing Agency
Scope Related to Vaccines
18 U.S.C. § 3486
Department of Justice (DOJ)
Investigations of “Federal health care offenses”. Used to seize records and compel custodian testimony regarding vaccine fraud.
5 U.S.C. § 406
HHS-OIG
Broad power to subpoena all information necessary to perform audits and investigations of HHS programs, including the vaccine supply chain.
21 U.S.C. § 372
FDA
While more regulatory, it empowers the FDA to conduct inspections and audits of vaccine manufacturing facilities.
18 U.S.C. § 3486(a)(1)(A)
FBI
Authorizes the FBI to issue administrative subpoenas specifically for health care fraud investigations, including those involving medical countermeasures.
Explanation: This table highlights the statutory backbone of federal investigative authority. These laws empower agencies to bypass traditional litigation hurdles and act quickly in cases of suspected fraud. Because vaccines are tied to federally funded programs, fraudulent activity falls squarely within these provisions. This legal infrastructure ensures swift accountability, but Kennedy’s administration failed to activate it.
Summary Table Of Federal Investigative Tools (Vaccine Context)
Tool
Status under Kennedy (Federal)
Civil Investigative Demand (CID)
Denied/Unconfirmed. No public record or official confirmation of use for vaccines.
Administrative Subpoena
Denied/Unconfirmed. No public record or official confirmation of use for vaccines.
Regulatory Mandate
Stayed/Superseded. The January 2026 schedule overhaul was stayed by Judge Murphy on March 16, 2026. The 2025 placebo trial mandate was superseded by the February 2026 “Single Pivotal Trial” standard.
Explanation: This table underscores the gap between authority and execution. Despite possessing powerful investigative tools, Kennedy’s administration did not deploy them effectively. Regulatory mandates were blocked by courts, and investigative powers remained unused. This failure highlights the difference between possessing authority and exercising it, leaving vaccine immunity intact and accountability mechanisms dormant.
Conclusion
The investigative arsenal available to federal and state governments represents a formidable counterweight to statutory immunity. CIDs, administrative subpoenas, and grand jury subpoenas could have been deployed to expose misconduct and build the evidentiary record necessary to overcome PREP Act protections. Yet Kennedy’s administration chose symbolic maneuvers over substantive enforcement, leaving these tools unused and preserving immunity. This failure was not due to a lack of legal authority but a political unwillingness to confront entrenched pharmaceutical interests. The consequence is clear: vaccine immunity remains intact, accountability has been sacrificed, and the promise of justice for the vaccine‑injured has been denied. History will judge Kennedy’s tenure as one of missed opportunities, where the most powerful tools of governance lay dormant in the face of public need.
The Advisory Commission on Childhood Vaccines (ACCV), statutorily established by the National Childhood Vaccine Injury Act of 1986, functions as a specialized stakeholder advisory body to the Secretary of Health and Human Services on the administration of the Vaccine Injury Compensation Program. Unlike the expertise-driven Advisory Committee on Immunization Practices (ACIP), the ACCV’s membership, purpose, and operational framework are rigidly defined by congressional statute rather than administrative discretion. This article provides a comprehensive examination of the ACCV’s legal foundations, contrasting its structure with that of ACIP, delineating the precise boundaries of the HHS Secretary’s authority over appointments, dismissals, and charter administration, and assessing the commission’s current functional limitations as of April 2026.
Drawing exclusively from the governing statutes, procedural mandates under the Federal Advisory Committee Act (FACA), and the documented administrative realities, the analysis demonstrates that while the Secretary retains broad discretion to select individuals within congressionally prescribed categories and to manage procedural elements of the charter, substantive changes to membership composition, mission, or authority remain the exclusive province of Congress. Comparative tables illuminate these distinctions and highlight the parallel yet distinct mechanisms by which both ACCV and ACIP have been rendered operationally constrained—ACIP by judicial order and ACCV by quorum deficiencies resulting from recent member dismissals. The article further explores the legal pipeline linking ACIP recommendations to the Vaccine Injury Table and the strictly advisory character of ACCV recommendations, which carry no binding force on the Secretary.
In the current environment of administrative flux, the ACCV continues to exist and deliberate but lacks the capacity for valid votes or formal recommendations, underscoring a deliberate statutory design that prioritizes balanced stakeholder representation over rapid executive adaptability. The discussion concludes that restoring full functionality to the ACCV will require the Secretary to exercise appointment authority within statutory limits, while any fundamental reform of the commission’s framework demands legislative action. This portrait of the ACCV reveals both its enduring value as a congressionally mandated forum for parents, attorneys, health professionals, manufacturers, and public health officials and the practical challenges of maintaining its statutory integrity amid ongoing operational constraints.
Introduction
The Advisory Commission on Childhood Vaccines (ACCV) stands as a distinctive statutory creation within the Department of Health and Human Services (HHS), born directly from the National Childhood Vaccine Injury Act of 1986. Enacted to establish the Vaccine Injury Compensation Program, the Act explicitly defined the ACCV’s membership categories, purpose, and advisory functions to ensure balanced representation of those most directly affected by vaccine policy: parents of vaccine-injured children, attorneys representing petitioners, health professionals including pediatricians, vaccine manufacturers, and public health officials. This deliberate stakeholder model distinguishes the ACCV from other advisory bodies and embeds it firmly within the Public Health Service Act while subjecting it to the transparency and balance requirements of the Federal Advisory Committee Act (FACA).
Congress crafted the ACCV not as an expert scientific panel but as a specialized forum where diverse perspectives could inform the administration of the compensation program. Appointments rest exclusively with the Secretary of HHS, who must select individuals fitting the statutorily enumerated categories; no additional categories may be created, nor may the balance be altered without congressional amendment. The commission advises on the Vaccine Injury Table and related policies, yet its recommendations remain strictly advisory. The Secretary is obligated to consult the ACCV before amending the Table but retains ultimate decision-making authority, provided procedural safeguards—such as notice-and-comment rulemaking—are observed.
As of April 2026, the ACCV operates in a state of partial functionality. Recent dismissals of several members have left the commission below the quorum threshold of five active voting members, preventing valid meetings or formal recommendations. Although the commission continues to meet and deliberate, its outputs lack enforceable weight. This situation parallels constraints affecting the related ACIP but arises from a distinct statutory mechanism: quorum failure rather than judicial intervention. The interplay between the two bodies remains critical; ACIP recommendations for routine childhood or maternal immunization serve as the prerequisite for inclusion on the Vaccine Injury Table that the ACCV helps oversee. Yet the ACCV’s charter is “locked” by statute in ways ACIP’s is not, limiting the Secretary’s ability to rewrite its fundamental structure.
This article confines its analysis strictly to the material at hand, exploring the ACCV’s statutory foundations, its procedural and structural distinctions from ACIP, the bounded nature of Secretarial authority, and the commission’s current operational realities. Through detailed examination of comparative tables and legal delineations, it illuminates how Congress’s deliberate design continues to shape the ACCV’s role even amid administrative transitions and quorum challenges.
Foundational Divergences: Core Structural and Procedural Distinctions Between ACIP and ACCV
The following table distills the essential statutory and operational contrasts that define the ACCV’s unique place within the federal advisory landscape, emphasizing how its framework was intentionally crafted by Congress to differ from the more flexible, expertise-oriented model of the ACIP.
Table 1: Key Differences Between ACIP And ACCV
Feature
ACIP
ACCV
Law
Public Health Service Act + FACA
National Childhood Vaccine Injury Act (1986)
Purpose
Advises CDC/HHS on vaccine schedules & recommendations
Advises HHS on Vaccine Injury Compensation Program
Appointments
Secretary of HHS (expert-based)
Secretary of HHS (statutorily defined categories)
Congress Role
Created statutory authority, oversight only
Created statutory authority, oversight only
Procedural Rules
FACA compliance (balance, transparency)
Statutory membership categories mandated
This table highlights the structural and procedural differences between the two advisory bodies. ACIP is primarily science- and expertise-driven, with appointments focused on medical and public health professionals under FACA’s balance requirements. ACCV, by contrast, is designed to represent a broader set of stakeholders—including families, lawyers, and manufacturers—because its role is tied to the Vaccine Injury Compensation Program. Congress set up both frameworks but does not participate in the appointment process, leaving that responsibility to HHS.
It underscores that the ACCV’s statutorily mandated categories ensure a permanent voice for vaccine-injured families and legal representatives, a feature absent from ACIP’s expert-based model. This design reflects Congress’s intent to balance scientific input with lived experience and stakeholder accountability in compensation matters. It also notes that while both commissions fall under FACA’s transparency umbrella, the ACCV’s procedural rules are more prescriptive, locking membership composition into law and thereby constraining administrative flexibility in ways that do not apply to ACIP.
Paralysis Parallels: Embargo Effects On Advisory Capacities
The next table provides a side-by-side snapshot of how judicial and quorum-related constraints have similarly diminished the practical authority of both bodies despite their continued legal existence and ongoing meetings.
Table 2: Comparative Snapshot Under Embargo
Feature
ACIP
ACCV
Charter Status
Renewed through April 2028
Ongoing under HRSA
Embargo Effect
Court ruling halted recommendations
Lack of quorum prevents valid votes
Current Functionality
Meets but cannot issue binding guidance
Meets but outputs are advisory only
Impact
Vaccine schedule updates frozen
Compensation policy advice weakened
This table shows that although the mechanisms differ—ACIP halted by judicial ruling, ACCV limited by quorum gaps—the functional outcome is the same: both bodies are unable to exercise their full statutory authority. They continue to exist and deliberate, but their recommendations are either suspended or downgraded to advisory status, leaving HHS without the usual formal input from these commissions.
Analysis of the table reveals that the ACCV’s current inability to achieve quorum stems directly from member dismissals earlier in 2026, rendering it non-functional for valid votes even as it continues to meet. This creates a temporary loss of the statutorily required advisory channel for stakeholders. Analysis also reveals that, unlike ACIP’s court-imposed freeze, the ACCV’s constraint is administrative in origin yet equally effective in weakening compensation policy input, highlighting how both commissions—despite different legal triggers—find themselves in parallel states of advisory limbo as of April 2026.
Navigating Permissible Bounds: Secretary’s Capacities And Constraints Over ACCV
This table delineates the precise administrative latitude granted to the HHS Secretary under the National Childhood Vaccine Injury Act and FACA, clarifying what remains beyond executive reach.
Table 3: Scope Of Secretary’s Authority
Area
Secretary Can Do
Secretary Cannot Do
Charter Renewal
Renew ACCV charter every 2 years under FACA
Eliminate ACCV or extend beyond statutory limits
Procedural Rules
Adjust meeting schedules, reporting formats, administrative support
Change statutory membership categories or quorum rules
This table shows the distinction: the Secretary’s authority is administrative and procedural, not legislative. ACCV’s charter can be updated in form, but its substance—membership categories, quorum requirements, and statutory mission—are fixed by law. Thus, the Secretary cannot unilaterally rewrite ACCV’s charter in a way that changes its legal foundation; only Congress can do that.
The analysis demonstrates that the Secretary possesses meaningful tools for day-to-day management—renewing the charter biannually and refining operational procedures—yet these powers stop short of altering the commission’s congressionally mandated composition or core functions. The analysis also emphasizes that this deliberate limitation protects the ACCV’s stakeholder balance from executive overreach, ensuring that any substantive evolution of the commission requires legislative action rather than administrative fiat.
Precision In Personnel: Statutory Slots And Secretarial Selection
The table below clarifies the Secretary’s appointment and dismissal authority, illustrating both its breadth within defined categories and its strict confinement by law.
Table 4: Secretary’s Appointment And Dismissal Authority
Area
Secretary Can Do
Secretary Cannot Do
Appointments
Select individuals within the statutory categories
Add new categories or appoint outside them
Dismissals
Remove members and appoint replacements
Remove categories or alter statutory balance
Discretion
Choose among eligible candidates
Override Congress’s statutory framework
Quorum Impact
Fill vacancies to restore quorum
Ignore quorum rules or bypass statutory requirements
This table shows that the Secretary’s authority is both powerful and constrained. He or she can appoint and dismiss members, but only in line with the categories Congress mandated. The Secretary cannot rewrite the law or redefine the Commission’s composition—only Congress can do that. In practice, this means the Secretary controls the individuals but not the structure of ACCV.
Examination of the table confirms that the Secretary retains significant influence over the ACCV’s composition by selecting qualified individuals for the fixed statutory slots—including two parents of vaccine-injured children, two attorneys, three health professionals, one manufacturer representative, and one public health official—and by addressing vacancies to restore quorum. The examination also notes, however, that recent dismissals have produced the current below-quorum status, illustrating how personnel decisions directly affect functionality while remaining powerless to expand or contract the categories themselves.
Governance Paradigms: Charter Flexibility In ACIP Versus Statutory Entrenchment In ACCV
This final table contrasts the administrative malleability of ACIP’s charter with the congressionally entrenched nature of the ACCV’s, underscoring a fundamental legal irony in their respective governance.
Table 5: Charter Authority Comparison
Feature
ACIP Charter
ACCV Charter
Legal Basis
Public Health Service Act + FACA
National Childhood Vaccine Injury Act (1986)
Secretary’s Appointment Power
Broad discretion to appoint experts
Limited to statutory categories defined by law
Charter Flexibility
Can be renewed/amended administratively
Fixed by statute; only Congress can change
Dismissal Authority
Secretary can remove/replace members
Secretary can remove/replace but only within categories
Structural Control
Secretary controls composition balance
Congress controls composition categories
This table highlights the key difference: ACIP’s charter is an administrative instrument that the Secretary can shape within FACA’s framework, while ACCV’s charter is a statutory creation that the Secretary cannot rewrite. In practice, this means ACIP is more adaptable to administrative priorities, whereas ACCV is bound tightly to the legislative framework Congress enacted.
The table reveals that the ACCV’s charter rigidity serves as a deliberate safeguard, preventing unilateral executive redesign of its stakeholder model even as the Secretary retains authority to appoint and dismiss within existing slots. The table also outlines the resulting irony: greater Secretarial flexibility over ACIP indirectly influences the Vaccine Injury Table through routine-use recommendations, yet the ACCV itself remains structurally insulated, requiring congressional action for any fundamental alteration.
Synergistic Yet Distinct: The Interconnected Roles Of ACIP And ACCV In Vaccine Policy
The legal pipeline between the two bodies is clear: an ACIP recommendation for routine administration establishes the prerequisite for a vaccine’s inclusion on the Vaccine Injury Table managed under ACCV oversight. While the ACCV provides specialized advice on compensation policy, its recommendations hold no legal power to compel the Secretary. The Secretary may amend the Table through notice-and-comment rulemaking after mandatory consultation with a functioning ACCV, but procedural formalities—including the 180-day comment period—must be observed. As of mid-April 2026, the absence of ACCV quorum, combined with the ACIP’s judicial stay, has stalled new initiatives, leaving the Secretary managing existing records and pre-existing schedules rather than advancing overhaul proposals. This interdependence underscores the ACCV’s role as a statutory check that, while advisory, ensures stakeholder perspectives remain formally recorded even when operational capacity is diminished.
Conclusion
The Advisory Commission on Childhood Vaccines remains a congressionally designed institution whose statutory rigidity continues to define its identity and limits even in 2026. Its membership categories, advisory mandate, and procedural requirements—explicitly fixed by the National Childhood Vaccine Injury Act of 1986—cannot be rewritten by the Secretary of HHS, who possesses only administrative and personnel authority within those boundaries. The comparative analyses presented demonstrate that the ACCV’s stakeholder-driven model, while more prescriptive than ACIP’s expertise-based structure, has produced parallel functional constraints: quorum failure has rendered the ACCV unable to issue valid recommendations, mirroring ACIP’s judicially frozen status.
Restoration of full ACCV functionality hinges on the Secretary’s prompt exercise of appointment powers to achieve quorum, thereby re-enabling formal consultation on Vaccine Injury Table matters. Yet any deeper reform—altering categories, mission, or charter substance—resides exclusively with Congress. In the current administrative landscape, the ACCV thus serves as both a vital forum for balanced perspectives and a statutory sentinel against unchecked executive redesign. Its continued existence, even in diminished form, affirms Congress’s original intent: to embed diverse voices permanently into the compensation framework. Until vacancies are filled and procedural stability restored, the commission’s advisory outputs will remain limited, underscoring the enduring truth that the ACCV’s strength lies not in binding power but in its legislatively guaranteed role as a transparent, stakeholder-inclusive voice within the nation’s vaccine injury compensation system.
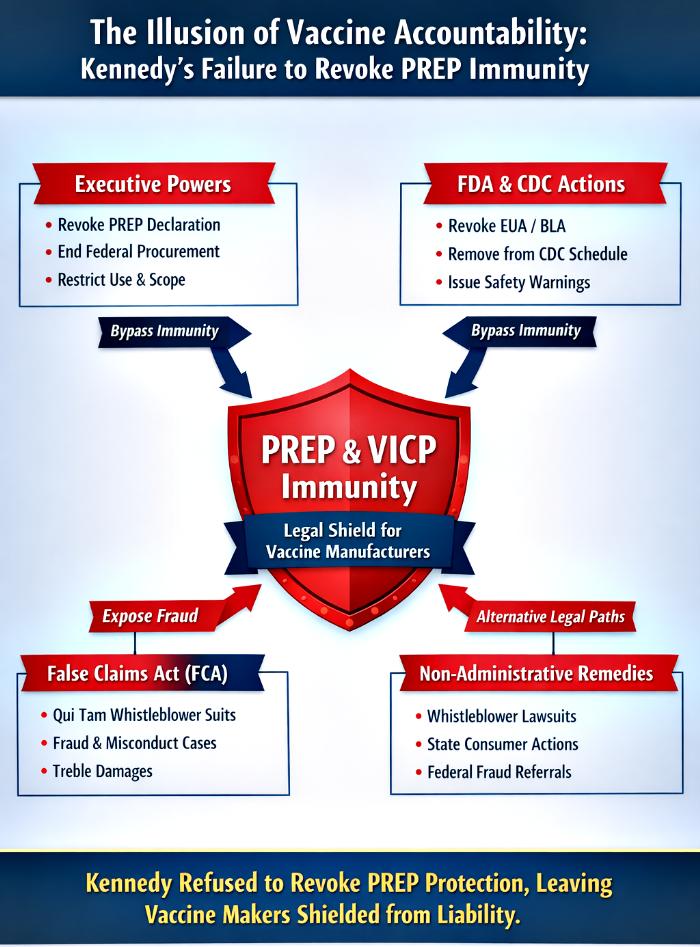
The liability architecture for vaccine manufacturers in the United States is dominated by two statutory regimes: the Public Readiness and Emergency Preparedness (PREP) Act and the National Childhood Vaccine Injury Act (NCVIA), which established the Vaccine Injury Compensation Program (VICP). These frameworks grant sweeping immunity to manufacturers, channeling claims into specialized compensation systems. Yet both contain pathways—executive, administrative, and judicial—that can prospectively or retrospectively strip immunity.
This article examines the full spectrum of powers available to Secretary Kennedy under the separation of powers doctrine: executive authority through PREP declarations, administrative oversight via FDA and CDC, quasi‑judicial enforcement through penalties and investigations, and parallel remedies such as the False Claims Act (FCA). It demonstrates that Kennedy possessed direct and effective tools to revoke immunity but instead chose a procedurally flawedACIP maneuver that predictably collapsed under judicial review in AAP v Kennedy. He is still following the same script without actually doing anything to safeguard the interests of US citizens.
By mapping these pathways and analyzing their implications, the article argues that Kennedy’s refusal to exercise his strongest executive lever—the revocation of the PREP Declaration—represents a profound failure of governance. The result is continued protection for vaccine manufacturers, leaving citizens reliant on weaker remedies such as FCA suits, whistleblower actions, and state consumer claims.
Introduction
Constitutional governance rests on the separation of powers: legislatures make laws, executives enforce them, and judiciaries interpret them. Within this framework, vaccine liability regimes in the United States balance two imperatives: incentivizing rapid vaccine development and ensuring accountability for misconduct. The PREP Act grants broad immunity to manufacturers of designated countermeasures, while the NCVIA channels injury claims into the VICP.
Yet immunity is not absolute. The Secretary of Health and Human Services (HHS) can revoke or amend PREP declarations, FDA can withdraw authorizations, CDC can alter immunization schedules, quasi‑judicial enforcement can expose misconduct, and the False Claims Act provides a parallel fraud‑based enforcement channel. These mechanisms bypass statutory channeling and open the door to traditional litigation.
Despite possessing these tools, Secretary Kennedy chose not to revoke the PREP Declaration for COVID vaccines—the most direct and effective pathway to strip immunity. Instead, he pursued a controversial ACIP maneuver that lacked procedural legitimacy and was stayed in AAP v Kennedy. This article dissects Kennedy’s available powers, his actual actions, and the consequences of his failure.
Remedies Through Executive, Administrative, And Quasi‑Judicial Powers
Table 1 — EAQ Powers Of Secretary Kennedy
Executive Powers
Administrative Powers
Quasi‑Judicial Powers
Issue or revoke PREP Act declarations (direct authority to grant/remove immunity).
FDA withdrawal of EUA/BLA; CDC/ACIP schedule changes.
Impose fines, penalties, sanctions; launch investigations into fraud or concealment.
Narrow scope of PREP declaration (limit persons, uses, geography).
HRSA programmatic delisting or prioritization changes in VICP intake.
Refer cases for criminal prosecution; support whistleblower suits.
Stop federal procurement or remove vaccines from federal programs.
Enable retrospective liability through misconduct findings.
Discussion:
Kennedy’s executive authority under the PREP Act was the most direct lever—a simple revocation of the COVID vaccine declaration would have stripped immunity instantly. Administrative tools such as FDA withdrawal or CDC schedule changes were secondary but still potent. Quasi‑judicial enforcement could expose fraud and misconduct, feeding evidence into litigation. Together, these powers formed a comprehensive arsenal to dismantle vaccine immunity.
Analysis:
(1) Executive Primacy: The PREP Declaration functions as an on/off switch for immunity. Kennedy’s refusal to revoke it represents a conscious abdication of responsibility.
(2) Administrative Support: FDA and CDC actions could have narrowed immunity, but Kennedy relied on ACIP theatrics that collapsed under judicial scrutiny.
(3) Quasi‑Judicial Enforcement: Investigations and penalties remain underutilized, leaving misconduct unpunished and immunity intact.
FDA And CDC Administrative Pathways
Table 2 — FDA And CDC Remedies
FDA Actions
CDC/ACIP Actions
Procedural Requirements
Withdraw or revoke EUA/BLA for vaccines.
ACIP votes to remove vaccine from immunization schedule; CDC adopts recommendation.
Must follow proper administrative procedure: notice, comment, scientific review.
Narrow indications or relabel vaccines.
Issue CDC guidance narrowing schedule inclusion.
Failure to follow procedure leads to judicial stay (AAP v Kennedy).
Issue enforcement letters, warning notices, or safety advisories.
Adjust HRSA/CDC programmatic intake prioritization for VICP claims.
Courts intervene if due process or statutory mandates are violated.
Discussion:
FDA and CDC wield indirect but significant powers. Withdrawal of authorizations or removal from immunization schedules reshapes the liability landscape by narrowing contexts where immunity applies. However, these actions require strict adherence to administrative procedure. Kennedy’s reliance on ACIP votes without procedural compliance guaranteed judicial invalidation.
Analysis:
(1) FDA Leverage: Withdrawal of EUA/BLA would have removed COVID vaccines from authorized use, exposing manufacturers to liability. Kennedy did not pursue this.
(2) CDC Fragility: ACIP votes are procedurally vulnerable. Kennedy’s reliance on this mechanism was a calculated but hollow gesture.
(3) Judicial Oversight: Courts swiftly stayed Kennedy’s ACIP maneuver, underscoring the futility of bypassing procedural safeguards.
False Claims Act: A Parallel Enforcement Channel
Table 3 — False Claims Act Remedies
Mechanism
Actor
Effect on Immunity
Evidence Needed
Practical Consequence
FCA civil action (qui tam or DOJ suit)
DOJ, whistleblowers
Does not directly revoke PREP/VICP immunity but exposes fraud outside those regimes
False billing records, misrepresentation of safety/efficacy, concealment of adverse data
Treble damages, civil penalties, evidentiary record supporting fraud/misconduct claims
Strengthens plaintiffs’ ability to argue fraud defeats statutory channeling
DOJ enforcement
Federal prosecutors
Parallel enforcement outside PREP/VICP
Criminal referrals, administrative findings
Adds weight to judicial findings that can strip immunity retrospectively
Discussion:
The FCA bypasses PREP and VICP entirely because it targets fraud against the government, not personal injury claims. Successful FCA actions produce robust evidence of fraud—internal emails, falsified submissions, suppressed adverse data—that courts can use to retrospectively defeat PREP or VICP immunity.
Analysis:
(1) Independent Enforcement Channel: FCA suits operate outside statutory channeling, making them one of the few remedies immune to PREP/VICP barriers.
(2) Evidentiary Bridge: FCA findings create the factual predicate for courts to pierce immunity in related injury cases.
(3) Instrumental In Parallel Tort Claims The FCA enables tort liability by creating a statutory mechanism that both proves and channels civil wrongdoing—its elements (a false representation, materiality, presentment to the government, and scienter) mirror common-law fraud elements so a successful FCA case often supplies the core factual and evidentiary predicates for parallel tort claims (fraud, conspiracy, unjust enrichment); additionally, qui tam proceedings unlock expansive pre-trial discovery and can produce judicial findings on falsity and intent that support collateral tort actions or equitable remedies, while state-law claims can be asserted alongside or where federal coverage is incomplete to capture private harms and restitution beyond the FCA’s statutory remedies.
Non‑Administrative Remedies: The Last Resort
Citizens now face reliance on weaker remedies outside the executive and administrative sphere:
(2) State consumer protection actions challenging deceptive practices.
(3) Federal enforcement referrals generating evidentiary records for litigation.
These remedies are reactive, slow, and dependent on judicial findings of fraud or misconduct. They lack the immediacy of executive revocation and rarely succeed in stripping immunity.
Conclusion
Secretary Kennedy possessed the most powerful tool to dismantle vaccine manufacturer immunity: revocation of the PREP Declaration for COVID-19 shots. This action required no legislative approval and would have instantly exposed manufacturers to traditional tort liability. Instead, Kennedy staged a symbolic ACIP maneuver that predictably collapsed under judicial review.
By refusing to exercise his executive authority, Kennedy has failed U.S. citizens and betrayed his core voters. His administration remains aligned with the vaccine lobby, preserving immunity and shielding manufacturers from accountability. The result is a liability regime where citizens must rely on weak remedies—FCA suits, whistleblower actions, and state consumer claims—while the pharmaceutical cartel continues to dominate.
Kennedy’s failure is not procedural—it is political. He chose drama over substance, optics over accountability, and lobby interests over public trust. The consequence is clear: vaccine immunity remains intact, and the promise of accountability has been sacrificed. The verdict of history will be unforgiving.
In these dark times of medical tyranny, systemic gaslighting, and the denial of remedies to the vaccine-injured, the HVBI Framework emerges as a guiding light. The path forward is clear—let the HVBI Framework illuminate the way.
The legal architecture surrounding vaccine manufacturer liability in the United States is shaped primarily by two statutory regimes: the Public Readiness and Emergency Preparedness (PREP) Act and the National Childhood Vaccine Injury Act (NCVIA), which created the Vaccine Injury Compensation Program (VICP). These frameworks provide broad immunity to manufacturers, channeling claims into specialized compensation systems. Yet, both statutes contain mechanisms—administrative and judicial—that can prospectively or retrospectively narrow or remove immunity.
This article explores the administrative pathways available to federal agencies to prospectively limit immunity under the PREP Act and VICP, the judicially enforced willful‑misconduct exception under PREP, and the doctrinal routes to retrospective defeat of VICP channeling. It also examines how whistleblower actions, state consumer protection suits, and federal enforcement interact with these immunities. By mapping these pathways, the article highlights the interplay between executive discretion, regulatory enforcement, and judicial oversight in shaping the liability landscape for vaccine manufacturers. Ultimately, while prospective removal of immunity is largely an administrative prerogative, retrospective defeat requires judicial findings of fraud or misconduct, underscoring the evidentiary and procedural hurdles that plaintiffs face.
Introduction
Vaccine liability regimes in the United States balance two competing imperatives: incentivizing rapid development and deployment of vaccines, particularly in emergencies, and ensuring accountability for misconduct or harm. The PREP Act grants sweeping immunity to manufacturers and distributors of designated countermeasures, while the NCVIA channels most vaccine injury claims into the VICP, a no‑fault compensation system. These frameworks are designed to stabilize markets and encourage innovation by limiting exposure to tort litigation. However, immunity is not absolute. The PREP Act allows the Secretary of Health and Human Services (HHS) to prospectively grant or revoke immunity through declarations, and it contains a narrow willful‑misconduct exception that permits retrospective liability. Similarly, while VICP channeling is statutory, courts can retrospectively defeat its protections in cases of fraud or intentional wrongdoing. This article systematically examines these pathways, situating them within broader administrative and judicial processes, and considers how external mechanisms—whistleblower suits, state enforcement, and federal penalties—interact with and erode these immunities.
Administrative Pathways To Prospectively Remove Or Limit Immunity
Table 1 — Administrative Pathways Under PREP And VICP
The first table maps the administrative instruments available to federal agencies to prospectively alter manufacturer immunity. It distinguishes between direct powers, such as the HHS Secretary’s PREP declaration, and indirect levers, such as FDA withdrawal of authorization or CDC schedule changes.
Administrative Action
Agency / Actor
Direct vs Indirect
Legal Effect (prospective)
Typical Mechanism / Form
Practical Result on Manufacturer Liability
Issue PREP Act declaration naming product
HHS Secretary
Direct
Grants broad prospective immunity for covered uses/persons/time (except willful misconduct)
Presidential/Secretary declaration under PREP Act (written declaration)
Strong, immediate immunity for future deployments covered by declaration
Amend or revoke PREP declaration to exclude product
HHS Secretary
Direct
Removes or narrows PREP immunity prospectively for specified uses/persons/time
Amendment or revocation of PREP declaration
PREP protection removed for future uses; manufacturers exposed to non‑PREP legal regimes
Combined effect: no PREP coverage; no FDA authorization for routine uses; no CDC schedule inclusion; no federal procurement — maximizes prospective liability exposure
Manufacturer effectively loses both PREP and practical VICP protection for future uses; exposed to ordinary tort/regulatory risk
Analysis
(1) The PREP Act declaration is the most direct administrative lever, functioning as an on/off switch for immunity. Revocation or amendment by the HHS Secretary immediately alters the liability landscape.
(2) Indirect mechanisms, such as FDA withdrawal or CDC schedule changes, reshape the regulatory and programmatic context, narrowing the scope of immunity without directly altering statutory coverage.
(3) The most robust strategy involves coordinated multi‑agency action, combining PREP revocation, FDA withdrawal, ACIP delisting, and procurement cessation. This sequence maximizes liability exposure by severing both statutory emergency immunity and programmatic protections tied to VICP.
Willful‑Misconduct Exception Under The PREP Act
Table 2 — Judicial Pathways To Retrospective Liability
The second table outlines the willful‑misconduct exception under the PREP Act, the only doctrinal gateway to retrospective removal of immunity. It requires clear and convincing evidence of intentional wrongdoing or conscious disregard of known risks.
Topic
Description
Legal Effect (retrospective/prospective)
Proof Standard & Elements
Typical Evidence
Practical Consequence for Immunity
Core rule
PREP grants broad immunity to covered persons, but immunity does not apply to conduct amounting to “willful misconduct.”
Retrospective for proven wrongful acts; prospective immunity remains for other covered acts unless proven otherwise
Clear and convincing evidence that covered person committed willful misconduct
Internal communications, safety data concealment, deliberate deviations from protocols, regulatory‑submission falsification
Immunity is void as to the specific willful misconduct acts — plaintiffs may sue for damages tied to those acts
Legal elements (typical judicial framing)
1) Affirmative act/omission (not mere negligence) 2) Actual intent to cause harm or conscious disregard of a known, substantial risk 3) Proximate causation of injury 4) Misconduct outside ordinary discretionary response covered by PREP
Retrospective application limited to established acts meeting elements
Clear and convincing; courts require specific proof of intent or conscious indifference
Documentary proof of awareness of risk; emails showing intent; meeting notes; manufacturing alterations; suppressed adverse event reports
If elements met, PREP immunity is treated as inapplicable to those acts; remedies follow ordinary tort law for those claims
Burden & difficulty
High evidentiary burden; plaintiffs must show mental state and causation beyond ordinary negligence
Makes retrospective loss of immunity possible but hard to obtain
Successful proof is rare but immediately exposes covered persons to retrospective liability for the proved acts
Analysis
(1) The willful‑misconduct exception is narrow but powerful. It pierces PREP immunity retrospectively for specific acts of intentional wrongdoing, allowing plaintiffs to pursue ordinary tort remedies.
(2) The evidentiary burden is high, requiring clear and convincing proof of intent or conscious disregard, supported by documentary evidence or whistleblower testimony.
(3) While rare, successful findings of willful misconduct carry severe consequences, including civil damages, administrative penalties, and potential criminal referrals, underscoring the deterrent effect of the exception.
Retrospective Defeat Of VICP Immunity
Table 3 — Judicial And Administrative Pathways Under NCVIA
The Vaccine Injury Compensation Program (VICP), established under the National Childhood Vaccine Injury Act (NCVIA), channels most vaccine injury claims into a specialized forum, limiting access to ordinary tort litigation. Unlike the PREP Act, which allows the HHS Secretary to prospectively revoke immunity, VICP protections are statutory and cannot be unilaterally removed by administrative action. The following table outlines the doctrinal pathways and actors involved in potentially defeating VICP immunity retrospectively.
Topic
VICP statutory scheme effect
Possible retrospective defeat?
Who can act (agency/actor)
Mechanism (administrative vs. judicial)
Typical evidence needed
Practical outcome if proven
Core structure
NCVIA channels most vaccine‑injury claims to VICP; petitioners generally must pursue VICP remedies rather than ordinary tort
Statute itself provides limited grounds to opt out or seek civil remedy; retrospective defeat of VICP immunity is possible only in narrow circumstances and typically via judicial findings, not mere agency fiat
Courts (Court of Federal Claims, federal trial courts) primarily; agencies (FDA, HHS/HRSA, CDC) can generate findings/facts that feed litigation but cannot unilaterally strip statutory channeling
Judicial determination that statutory requirements were not met or that misconduct defeats statutory protection; administrative findings (e.g., FDA enforcement actions, criminal convictions) supply evidence
Clear proof of fraud, concealment, willful misconduct, or procedural failures in VICP petitions; internal documents, altered safety data, regulatory submissions withholding
Court may permit civil suit or find statutory channeling inapplicable for the misconduct‑based claims; can produce retrospective liability for defendants
Fraud/Willful misconduct by manufacturer
VICP does not generally immunize for fraud or intentional wrongdoing; NCVIA contemplates some exceptions where ordinary remedies remain available
Retrospective defeat possible if fraudulent concealment or willful misconduct is judicially established
Plaintiffs in court; evidence often developed via discovery and supported by agency records
Judicial ruling that fraud/intentional misconduct falls outside protected conduct; criminal conviction strengthens case
Plaintiffs may pursue tort claims notwithstanding VICP channeling; VICP remedies may be bypassed for those claims
Procedural defects in VICP process
VICP requires petitioners to follow statutory procedures; agency misapplication may affect remedies
Procedural failures by program administrators generally do not abrogate statutory channeling; courts review but do not often open broad retrospective damages avenues
HRSA/Division of Injury Compensation Programs (DICP) administers VICP; courts review program decisions
Judicial review of VICP adjudication; rare vacatur or remand but not blanket removal of statutory scheme
Record showing procedural denial of rights or unlawful practice in adjudication
Relief usually limited to vacatur/remand or corrective administrative action, not wholesale opening of tort claims
Agency findings can be powerful evidence but do not themselves nullify NCVIA channeling
Agencies cannot unilaterally convert VICP claims into ordinary tort remedies; their findings enable judicial proceedings that may strip statutory protections for particular acts
FDA, HHS, CDC can investigate, suspend approvals, refer for criminal prosecution, issue public findings
Administrative enforcement, inspections, criminal referrals produce records used in civil litigation
Regulatory inspection reports, warning letters, criminal indictments, Official FDA determinations
If courts find willful misconduct/fraud based on such evidence, plaintiffs may be permitted ordinary suits for affected claims
Interaction with state law
NCVIA preemption is complex; certain state‑law claims can be preempted or barred by NCVIA’s scheme
Retroactive disapplication is rare; success depends on judicial interpretation and strength of misconduct evidence
Federal courts interpret preemption; state courts may see parallel claims depending on context
Preemption analysis in litigation; successful arguments can free some claims from channeling
Legal analysis, precedent, and fact pattern showing fraud/intentional conduct
Court may permit state‑law claims to proceed if not preempted; otherwise VICP remains exclusive route
Practical hurdles
High evidentiary bar; VICP is designed to centralize vaccine injury compensation and limit tort suits
Retrospective defeat is exceptional and fact‑specific; agency actions help but do not themselves flip channeling
Plaintiffs, discovery, and courts are central actors; agencies provide investigative materials
Litigation (often lengthy), discovery disputes, motion practice
Whistleblower disclosures, criminal cases, internal documents, agency enforcement records
Possible retrospective liability for proven wrongful acts, but usually limited in scope and hard to obtain
Analysis
Judicial Primacy
The VICP regime is fundamentally judicial in its retrospective defeat mechanisms. Courts, not agencies, determine whether statutory channeling applies in cases of fraud or misconduct. While agencies such as FDA or HHS can generate findings and evidence, they cannot themselves nullify VICP protections. Judicial rulings based on fraud, concealment, or willful misconduct are the only viable routes to bypass the statutory channeling and allow ordinary tort claims.
Evidentiary Burden
The most realistic path to retrospective defeat of VICP immunity lies in proving fraud or intentional wrongdoing. Plaintiffs must present compelling documentary evidence—internal communications, falsified regulatory submissions, or suppressed adverse event data. Agency enforcement actions, criminal referrals, or whistleblower disclosures often provide the factual predicate for such claims. Courts then apply these findings to determine whether statutory protections should be stripped for specific acts.
Practical Challenges
Despite the doctrinal possibility, retrospective defeat of VICP immunity remains rare. The statutory design favors centralization and predictability, and courts construe exceptions narrowly to preserve the program’s integrity. Discovery disputes, privilege claims, and complex causation issues further raise the barrier. Nevertheless, when plaintiffs succeed in producing robust evidence, courts can treat discrete wrongful acts as outside NCVIA’s channeling, permitting ordinary tort claims and retrospective liability. This underscores the limited but potent role of judicial oversight in balancing accountability with statutory immunity.
Conclusion
The interplay between administrative and judicial pathways reveals a layered liability framework for vaccine manufacturers. Prospective removal of immunity under the PREP Act is largely an executive function, with the HHS Secretary wielding direct authority through declarations. Retrospective defeat, however, is judicially driven: courts alone can pierce statutory protections under PREP’s willful‑misconduct exception or VICP’s fraud‑based exclusions.
Agencies play a critical supporting role by generating evidence through enforcement actions, inspections, and referrals, but they cannot unilaterally strip immunity. Whistleblower suits, state consumer actions, and federal enforcement further erode immunities by creating evidentiary records and collateral remedies. Ultimately, while the statutory schemes are designed to stabilize vaccine markets and encourage innovation, the pathways examined here ensure that accountability remains possible in cases of fraud, concealment, or intentional misconduct. This balance between protection and liability is essential to maintaining public trust in vaccination programs and regulatory institutions.
The Centers for Disease Control and Prevention (CDC) has constructed its HPV vaccination campaign upon three rhetorical pillars: universality, persistence, and vaccine efficacy. These claims, repeated in public health discourse, create a narrative of inevitability—that HPV is ubiquitous, that persistence is common and dangerous, and that vaccines are the only salvation. Yet when examined through biological plausibility, epidemiological trajectories, and immunological mechanisms, each pillar collapses under scrutiny. The HPV Vaccines Biological Impossibilities (HVBI) Framework and the Pointer–Eliminator Principle provide a coherent rebuttal, demonstrating that HPV infections are overwhelmingly rare and transient, persistence is vanishingly rare, and vaccines are biologically incapable of preventing infection or cancer. Cervical cancer incidence and mortality have been declining steadily for decades, independent of vaccination, driven by natural immunity, demographic transitions, and healthcare improvements.
Beyond scientific critique, the jurisprudential doctrines of Praveen Dalal—particularly the Unacceptable Human Harm Theory (UHHT) and the Oppressive Laws Annihilation (OLA) Theory—provide a moral and legal foundation for rejecting hollow assurances and dismantling immunity provisions that shield pharmaceutical corporations from accountability. UHHT asserts that any harm from medical interventions must trigger immediate liability, while OLA Theory demands the annihilation of laws that protect corporations over human lives. Together, these frameworks converge on a U.S.-specific remedy: embedding Absolute Liability for HPV vaccines into law, annulling immunity provisions, and ensuring enforceable rights for victims. This article synthesizes biological, epidemiological, and techno-legal critiques into a unified conclusion: the CDC’s HPV narratives are pseudoscientific, misleading, and ethically indefensible, while absolute liability and UHHT restore justice, accountability, and human dignity.
Introduction
HPV has been framed by the CDC as the “most common sexually transmitted infection,” with “some infections persisting and progressing to cancer,” and vaccines positioned as the decisive preventive tool. These claims, taken together, construct a narrative of inevitability: that nearly everyone is infected, many will persist, and vaccines are the only salvation. Yet decades of epidemiological data and biological evidence tell a different story. Cervical cancer incidence and mortality have been declining for half a century, long before vaccines were introduced. More than 95% of HPV infections clear naturally within 1–2 years, persistence occurs in fewer than 0.0005 of the population at any given time, and progression to cancer is rarer still. Vaccines, operating only as pointers under the Pointer–Eliminator Principle, cannot prevent infection or cancer.
At the same time, the U.S. legal system has failed to provide meaningful remedies for victims of vaccine injuries. Immunity provisions shield pharmaceutical corporations from accountability, leaving victims without enforceable rights. Paper assurances of safety, issued by agencies and medical boards, are ethically and legally unacceptable. The doctrines of UHHT and OLA Theory provide a jurisprudential foundation for rejecting these hollow assurances and demanding absolute liability for medical offenses.
Universality: The Collapse Of The “Most Common” Claim
The CDC’s universality claim exaggerates risk by conflating transient viral DNA detection with persistent oncogenic disease. In reality, only about 1% of the U.S. population is infected at any given time. Of those, 95% clear the infection naturally within 1–2 years. The remaining 5% of that 1% may show persistence, but even here, 4% clear at the CIN1/2 stage. That leaves only ~1% of 5% of 1% of the population—about 0.0005 overall—who are truly persistently infected. This mathematical breakdown dismantles the CDC’s universality narrative. If HPV were truly “universal,” catastrophic cancer rates would be observed. Instead, SEER data confirm that cervical cancer incidence and mortality have been declining steadily for decades, independent of vaccination.
Persistence: Vanishingly Rare And Misrepresented
The persistence narrative implies millions at risk of cancer, yet transparent statistics reveal persistence is vanishingly rare. Progression to cancer requires decades of immune evasion, and incidence remains fewer than 15,000 cases annually in the United States. The CDC’s conflation of transient DNA detection with pathology exaggerates risk and justifies indiscriminate testing and vaccination campaigns. If persistence were as common as claimed, millions of cancers would be expected annually. Instead, mortality continues to decline, driven by natural immunity, demographic transitions, and improved healthcare access.
Vaccine Efficacy: The Pointer–Eliminator Principle
The vaccine narrative collapses under both biological and epidemiological scrutiny. Vaccines and their dangerous antibodies function only as dangerous pointers, incapable of eliminating pathogens. True destruction is performed by immune effector mechanisms. Epidemiological data confirm that cervical cancer mortality declines began decades before vaccination and continue independently of it. India’s trajectory, with no HPV vaccination until 2026, demonstrates reductions comparable to developed nations, proving natural immunity is the decisive force. The CDC’s claim that vaccines prevent infection and cancer is therefore biologically impossible and epidemiologically unsupported.
Comparative Analysis: CDC Narratives Versus The HVBI Framework
A pivotal element in understanding the scientific invalidity of the CDC’s HPV vaccination campaign lies in the direct comparison between its core claims and the counter-evidence marshaled by the HVBI Framework. This table not only distills the essence of the debate into clear categories but also demonstrates how each pillar of the official narrative—universality, persistence, and vaccine efficacy—fails when subjected to rigorous biological, immunological, and epidemiological analysis. By presenting these contrasts, the table serves as a foundational tool for readers to appreciate the depth of the pseudoscientific foundations upon which current policies rest, thereby justifying the urgent need for jurisprudential remedies such as those proposed by UHHT, Absolute Liability, and OLA Theory to protect public health and human rights.
Aspect
CDC Claim
HVBI Framework Evidence
Universality
HPV is “most common STI”
Only ~1% of population infected at any given time; >95% clear naturally within 2 years
Persistence
“Some infections persist and progress”
Of the 1% infected, 95% clear; remaining 5% → 4% clear at CIN1/2 stage; only ~0.0005 persist
Vaccine Efficacy
Vaccines prevent infection and cancer
Vaccines are dangerous pointers only; elimination is immune‑driven; declines predate vaccination
Analysis: From Biological Critique To Jurisprudential Remedy
The CDC’s rhetorical pillars collapse when confronted with biological plausibility and epidemiological data. Universality is disproven by the fact that only 1% of the population is infected at any given time, with nearly all clearing naturally. Persistence is dismantled by the vanishingly small fraction of infections that truly persist, amounting to 0.0005 of the population. Vaccine efficacy is refuted by the Pointer–Eliminator Principle and decades of declining cancer rates independent of vaccination.
Yet scientific critique alone is insufficient. Victims of HPV vaccine injuries remain without justice because immunity provisions shield corporations from accountability. Here, jurisprudential doctrines provide the necessary remedy. The Unacceptable Human Harm Theory (UHHT) asserts that no medical intervention should cause any harm, and when such harm occurs, immediate legal consequences must follow. UHHT strengthens the case for Absolute Liability, ensuring that accountability is not delayed or diluted by bureaucratic promises. The Oppressive Laws Annihilation (OLA) Theory confronts the reality that laws protecting corporations over human lives are instruments of tyranny. OLA demands ignoring of oppressive laws by people, dismantling of immunity provisions, and annulling legal shields that perpetuate systemic injustice. Together, UHHT and OLA provide a techno‑legal foundation for embedding Absolute Liability into U.S. law, ensuring that victims are no longer burdened with proving negligence and that accountability is automatic, enforceable, and uncompromising.
The HVBI 12-Stage Framework: A Comprehensive Blueprint Exposing Pseudoscience And Charting The Path To Accountability
Building upon the biological and epidemiological critiques, the HVBI Framework provides a comprehensive 12-stage analysis that systematically deconstructs the pseudoscientific foundations of HPV vaccination campaigns from 1970 to 2026. This framework integrates insights from microabrasions, infection rates, immunity dynamics, and jurisprudential theories to offer not only a scientific rebuttal but also a practical roadmap for legal reform. The table below details each stage, illustrating how the framework progresses from identifying flawed assumptions to prescribing actionable remedies for victims of vaccine injuries, thereby equipping advocates, lawmakers, and citizens with the intellectual and legal tools necessary to challenge medical tyranny and restore enforceable human rights.
Laws protecting corporations over human lives perpetuate systemic injustice
Demands Legislative dismantling of immunity provisions and annulment of oppressive legal shields. If Govt fails, People must “Actively Disobey” such Oppressive Laws. When Injustice Becomes Law, Resistance Becomes Duty
The first six stages of the HVBI Framework form the biological foundation of its critique, systematically dismantling the pseudoscientific assumptions that have long underpinned HPV vaccine narratives. Stage 1 challenges the microabrasions presumption, showing that the supposed gateways for infection are exceedingly rare and not the universal entry points claimed by mainstream science. Stage 2 dismantles the near‑universal infection presumption, exposing how epidemiological data reveal that only about 1% of individuals are infected at any given time, with the vast majority clearing the virus naturally. Stage 3 confronts the unscientific risk presumption, demonstrating that natural clearance is not only safe but overwhelmingly effective, while vaccines themselves introduce severe adverse effects. Stage 4 critiques the claim that vaccines prevent infection, reframing them as biologically impossible interventions that act merely as strain‑specific alarms rather than shields. Stage 5 exposes the non‑efficacy of vaccines in reducing cancer rates, attributing observed declines instead to natural clearance and screening programs. Finally, Stage 6 introduces the Pointer–Eliminator Principle, a conceptual framework that clarifies how vaccines can only tag pathogens but never destroy them, leaving true protection to innate and adaptive immunity. Together, these stages establish a coherent biological rebuttal: HPV infections are transient, natural immunity is decisive, and vaccines are incapable of delivering the protection they promise.
Stages 7 and 8 expand the critique beyond biology into the epidemiological and ethical domains, revealing how narratives have been distorted and how coercive practices have undermined trust. Stage 7, the Epidemiological Narrative Distortion, demonstrates that long‑term declines in HPV‑related cancers predate the introduction of vaccines, driven instead by natural immunity, improved hygiene, and screening programs. This exposes how public health authorities have falsely credited vaccines with outcomes that were already in motion, misattributing causation and inflating their role in cancer prevention. Stage 8 escalates the framework into the ethical sphere, framing coercive vaccination campaigns as medical genocide and systemic ethical failure. Here, HVBI highlights how evidence of severe adverse effects and deaths has been suppressed, while natural immunity data has been ignored, creating a crisis of trust. Coercive campaigns, particularly those targeting young populations, are presented as deliberate acts of negligence and harm, undermining both public health credibility and the dignity of those subjected to them. These stages underscore that the HPV vaccine narrative is not only scientifically flawed but also ethically indefensible, built upon distortion and coercion rather than truth and transparency.
Stage 9 introduces a quantitative reframing through the Death‑to‑Population Ratio (DPR), a metric that contextualizes cervical cancer mortality relative to population size. Conventional metrics, which focus on raw death counts, exaggerate India’s cervical cancer burden and fuel fear‑driven narratives that justify coercive vaccination campaigns. DPR, by contrast, demonstrates that India’s proportional risk is comparable to that of developed nations, despite the absence of widespread screening, treatment, or vaccination until 2026. This reframing dismantles the rhetoric of crisis, showing that progress is real and that the proportional risk is low. By shifting the discourse from raw numbers to proportional analysis, DPR exposes how fear has been weaponized to push dangerous interventions while ignoring the reality of natural immunity and demographic transitions. It provides a more accurate, balanced, and humane perspective, proving that coercive vaccination campaigns are unjustified and that India’s trajectory reflects resilience and progress rather than vulnerability. Stage 9 thus completes the scientific and epidemiological dismantling of HPV vaccine narratives by grounding the debate in proportional truth rather than exaggerated fear.
The final three stages—10 through 12—extend the HVBI Framework into jurisprudence, embedding accountability and justice into the critique. Stage 10, the Unacceptable Human Harm Theory (UHHT), asserts that any harm from medical interventions is unacceptable and must trigger immediate liability. This doctrine rejects the notion that adverse effects can be tolerated or excused, demanding that human dignity and safety remain paramount. Stage 11, Absolute Liability, builds upon UHHT by embedding enforceable accountability into law, ensuring that victims of vaccine injuries are granted automatic rights without the burden of proving negligence. This dismantles the immunity provisions that currently shield pharmaceutical corporations, restoring justice and making accountability uncompromising. Stage 12, the Oppressive Laws Annihilation (OLA) Theory, confronts the systemic injustice of laws that prioritize corporate protections over human lives. OLA demands the dismantling of these oppressive legal shields, annulling immunity provisions, and ensuring that accountability is prioritized above corporate interests. Together, these jurisprudential doctrines transform the HVBI Framework from a scientific and ethical critique into a techno‑legal remedy, ensuring that vaccine safety is not a matter of paper assurances but a legally guaranteed right. By embedding absolute liability into law and annihilating oppressive protections, the framework restores justice, accountability, and human dignity, completing its comprehensive dismantling of pseudoscience, distortion, and systemic negligence.
Exposing The Sham Compensation System: The Financial Realities Of Vaccine Injuries And The Urgent Need For Systemic Reform
The absence of meaningful remedies for vaccine-injured individuals in the United States is starkly illustrated by the operational realities of the National Vaccine Injury Compensation Program (VICP) and related global market data. Far from delivering justice, this system reveals a profound structural imbalance in which pharmaceutical industry profits vastly outpace the meager compensation awarded to victims, perpetuating gaslighting, denial, and corporate impunity. The table below details petition filings, adjudication outcomes, compensation payouts, industry revenues, and insurance coverages for major vaccines over the 2015–2025 decade, providing irrefutable evidence of how even HPV vaccines—central to the CDC’s campaign—generate enormous profits while injured Americans receive only token relief under a framework that shields manufacturers from true accountability.
Table 1: Vaccine Petitions And Market Metrics (2015–2025)
This table details vaccine administration, adjudication outcomes, and revenue estimates for the last decade.
Vaccine Name
Petitions Filed
Petitions Allowed
Petitions Dismissed
Pending Cases
Comp. Paid (2015-25)
Industry Revenue (2015-25)
Insurance Coverage (2015-25)
Influenza
~7,800
~4,400
~2,500
~900
~$680 M
~$70 B
~$14 B
Pneumococcal
~350
~120
~140
~90
~$180 M
~$85 B
~$17 B
HPV
~190
~70
~75
~45
~$60 M
~$50 B
~$10 B
DTaP/Tdap
~690
~230
~320
~140
~$190 M
~$20 B
~$4 B
MMR
~480
~65
~340
~75
~$130 M
~$13 B
~$2.5 B
Hepatitis A/B
~420
~150
~180
~90
~$160 M
~$15 B
~$3 B
Meningococcal
~210
~80
~90
~40
~$90 M
~$18 B
~$3.5 B
Varicella
~115
~38
~50
~27
~$35 M
~$7 B
~$1.4 B
Rotavirus
~230
~90
~100
~40
~$110 M
~$9 B
~$1.8 B
Polio (IPV)
~28
~3
~20
~5
~$6 M
~$5 B
~$1 B
COVID-19*
~13,000
~15
~1,200
~11,700
~$25 M
~$180 B
~$36 B
Note: COVID-19 claims are managed by the CICP, which has a higher dismissal rate and lower payout threshold than the VICP.
Historical Dimensions Of The Compensation Crisis: Long-Term Profits, Payouts, And The Entrenchment Of Corporate Immunity
Extending this examination over the longer historical period since the program’s inception in 1988, the following table offers a longitudinal perspective on cumulative compensation, estimated industry profits, and insurance outlays. This broader view reinforces the systemic entrenchment of the problem, demonstrating how decades of liability protections have enabled vaccine manufacturers to amass extraordinary wealth while the public and injured individuals bear the overwhelming financial and human costs, further highlighting the oppressive legal architecture that UHHT and OLA Theory are designed to annihilate.
Table 2: Historical VICP, Profit, And Insurance Metrics (1988–2025)
This table compares long-term federal compensation against industry profits and insurance outlays.
Vaccine Name
Comp. Paid (2015-25)
Total Comp. (Since 1988)
Est. Profit (2015-25)
Est. Profit (Since 1988)
Est. Insurance (2015-25)
Est. Insurance (Since 1988)
Influenza
~$680 M
~$1.25 B
~$17.5 B
~$37.5 B
~$14 B
~$29 B
Pneumococcal
~$180 M
~$200 M
~$21.2 B
~$35.0 B
~$17 B
~$28 B
HPV
~$60 M
~$135 M
~$12.5 B
~$21.2 B
~$10 B
~$16 B
DTaP/Tdap
~$190 M
~$620 M
~$5.0 B
~$16.2 B
~$4 B
~$12 B
MMR
~$130 M
~$500 M
~$3.2 B
~$13.7 B
~$2.5 B
~$10 B
Hepatitis A/B
~$160 M
~$250 M
~$3.7 B
~$8.7 B
~$3 B
~$7 B
Meningococcal
~$90 M
~$120 M
~$4.5 B
~$7.0 B
~$3.5 B
~$5.6 B
Varicella
~$35 M
~$120 M
~$1.7 B
~$7.5 B
~$1.4 B
~$5.6 B
Rotavirus
~$110 M
~$160 M
~$2.2 B
~$4.5 B
~$1.8 B
~$3.6 B
Polio (IPV)
~$6 M
~$150 M
~$1.2 B
~$6.2 B
~$1 B
~$4.4 B
COVID-19*
~$25 M
~$25 M
~$45.0 B
~$45.0 B
~$36 B
~$36 B
Analysis Summary
The data reveals a stark contrast between the financial mechanisms of the vaccine industry and the federal compensation programs designed to protect the public. Here is the analysis of the relationship between industry profits, insurance burdens, and the VICP.
The Multi-Layered Financial Burden
The primary analysis shows that the financial burden of vaccine injuries is structured in layers, where the injured individual and the public taxpayer often shoulder the heaviest weight. Under federal law, insurance is the “first-payer,” meaning private insurance premiums and public taxes (funding Medicare/Medicaid) cover the immediate, high-cost medical bills, such as hospital stays and surgeries. Only after these primary funds are exhausted does the VICP step in to provide “gap-funding” for secondary costs like pain and suffering or lost wages. This creates a system where the public effectively co-funds the safety net through their own premiums while the VICP trust fund remains a secondary resource.
Profit vs. Compensation Imbalance
A significant disparity exists between the net profits of vaccine manufacturers and the total compensation awarded to victims. Since 1988, estimated industry profits for covered vaccines have reached approximately $204 billion, while total VICP compensation payouts over the same 37-year span total roughly $5.3 billion. This indicates a profit-to-compensation ratio where manufacturers retain roughly $38 in net profit for every $1 awarded to injured parties. This highlights a highly protected economic environment for the industry, where massive global revenues are shielded by significant liability protections.
The Role Of The Excise Tax Trust Fund
Unlike corporate profits, the VICP is funded entirely by a $0.75 excise tax per dose of vaccine. This fund has grown to a balance of approximately $4.5 billion, yet it remains separate from the manufacturer’s primary revenue streams. While the industry contributes through this tax, the data from 2015–2025 suggests that the volume of petitions—particularly for Influenza—is rising faster than the adjudication rate. This bottleneck in the “Special Masters” court often leaves petitioners waiting for years while the industry continues to see high-margin growth in newer sectors like HPV and Pneumococcal vaccines.
Settlement Trends And Adjudication Hurdles
The analysis of petitions shows that the majority of compensated cases (roughly 70% to 80%) are negotiated settlements. In these instances, the government pays the claimant without officially concluding that the vaccine caused the injury. This “no-fault” mechanism is intended to speed up the process, but it often results in lower payouts compared to traditional civil litigation. Furthermore, dismissal rates remain high, with approximately 60% of all petitions filed in the last decade being dismissed, often due to strict legal standards or lack of specific medical evidence required by the “Table of Injuries.”
The CICP And COVID-19 Discrepancy
A critical distinction in the 2015–2025 data is the separation of COVID-19 vaccines into the Countermeasures Injury Compensation Program (CICP). Despite generating an estimated $180 billion in revenue and $45 billion in profit globally, COVID-19 compensation remains negligible compared to the VICP. The CICP has a significantly higher bar for evidence and does not cover attorney fees or pain and suffering. This has led to a massive backlog of over 11,000 pending cases, highlighting a systemic imbalance where one of the most profitable vaccine rollouts in history has the most restrictive compensation pathway for the public.
Conclusion
The CDC’s three pillars—universality, persistence, and vaccine efficacy—are unscientific, pseudoscientific, and disconnected from ground reality. HPV infections occur rarely and are overwhelmingly cleared naturally, persistence is vanishingly rare, and vaccines are biologically incapable of preventing infection or cancer. Epidemiological data confirm that cervical cancer incidence and mortality have been declining for decades, independent of vaccination, driven by natural immunity and healthcare improvements.
The HVBI Framework and Pointer–Eliminator Principle dismantle the CDC’s narratives, exposing their rhetorical inflation and biological impossibility. But critique must be matched with remedy. The doctrines of UHHT and OLA Theory provide that remedy, demanding absolute liability for HPV vaccines and the annulment of immunity provisions that shield corporations from accountability. Vaccine safety must not remain a matter of paper assurances—it must be a legally guaranteed right. Only by embedding absolute liability into U.S. law can justice be real, accountability be immediate, and human harm never tolerated.
In these dark times of medical tyranny, systemic gaslighting, and the denial of remedies to the vaccine-injured, the HVBI Framework emerges as a guiding light. It offers not only a rigorous scientific and epidemiological rebuttal but also a powerful techno-legal pathway to justice, empowering the American people to reject hollow assurances, dismantle oppressive immunity shields, and secure absolute liability as an unassailable right. By embracing the HVBI Framework, the United States can transcend pseudoscience, restore human dignity, and lead the world toward a future where no injury is tolerated, no victim is abandoned, and accountability is the cornerstone of public health.
The path forward is clear—let the HVBI Framework illuminate the way.
The Centers for Disease Control and Prevention (CDC) has constructed its HPV vaccination campaign upon three rhetorical pillars: universality, persistence, and vaccine efficacy. These claims, repeated in public health discourse, create a narrative of inevitability—that HPV is ubiquitous, that persistence is common and dangerous, and that vaccines are the only salvation. Yet when examined through biological plausibility, epidemiological trajectories, and immunological mechanisms, each pillar collapses under scrutiny. The HPV Vaccines Biological Impossibilities (HVBI) Framework and the Pointer–Eliminator Principle provide a coherent rebuttal, demonstrating that HPV infections are overwhelmingly transient, persistence is vanishingly rare, and vaccines are biologically incapable of preventing infection or cancer. Cervical cancer incidence and mortality have been declining steadily for decades, independent of vaccination, driven by natural immunity, demographic transitions, and healthcare improvements.
Beyond scientific critique, the jurisprudential doctrines of Praveen Dalal—particularly the Unacceptable Human Harm Theory (UHHT) and the Oppressive Laws Annihilation (OLA) Theory—provide a moral and legal foundation for rejecting hollow assurances and dismantling immunity provisions that shield pharmaceutical corporations from accountability. UHHT asserts that any harm from medical interventions must trigger immediate liability, while OLA Theory demands the annihilation of laws that protect corporations over human lives. Together, these frameworks converge on a U.S.‑specific remedy: embedding absolute liability for HPV vaccines into law, annulling immunity provisions, and ensuring enforceable rights for victims. This article synthesizes biological, epidemiological, and techno‑legal critiques into a unified conclusion: the CDC’s HPV narratives are pseudoscientific, misleading, and ethically indefensible, while absolute liability and UHHT restore justice, accountability, and human dignity.
Introduction
HPV has been framed by the CDC as the “most common sexually transmitted infection,” with “some infections persisting and progressing to cancer,” and vaccines positioned as the decisive preventive tool. These claims, taken together, construct a narrative of inevitability: that nearly everyone is infected, many will persist, and vaccines are the only salvation. Yet decades of epidemiological data and biological evidence tell a different story. Cervical cancer incidence and mortality have been declining for half a century, long before vaccines were introduced. More than 95% of HPV infections clear naturally within 1–2 years, persistence occurs in fewer than 0.0005 of the population at any given time, and progression to cancer is rarer still. Vaccines, operating only as pointers under the Pointer–Eliminator Principle, cannot prevent infection or cancer.
At the same time, the U.S. legal system has failed to provide meaningful remedies for victims of vaccine injuries. Immunity provisions shield pharmaceutical corporations from accountability, leaving victims without enforceable rights. Paper assurances of safety, issued by agencies and medical boards, are ethically and legally unacceptable. The doctrines of UHHT and OLA Theory provide a jurisprudential foundation for rejecting these hollow assurances and demanding absolute liability for medical offenses.
Universality: The Collapse Of The “Most Common” Claim
The CDC’s universality claim exaggerates risk by conflating transient viral DNA detection with persistent oncogenic disease. In reality, only about 1% of the U.S. population is infected at any given time. Of those, 95% clear the infection naturally within 1–2 years. The remaining 5% of that 1% may show persistence, but even here, 4% clear at the CIN1/2 stage. That leaves only ~1% of 5% of 1% of the population—about 0.0005 overall—who are truly persistently infected. This mathematical breakdown dismantles the CDC’s universality narrative. If HPV were truly “universal,” catastrophic cancer rates would be observed. Instead, SEER data confirm that cervical cancer incidence and mortality have been declining steadily for decades, independent of vaccination.
Persistence: Vanishingly Rare And Misrepresented
The persistence narrative implies millions at risk of cancer, yet transparent statistics reveal persistence is vanishingly rare. Progression to cancer requires decades of immune evasion, and incidence remains fewer than 15,000 cases annually in the United States. The CDC’s conflation of transient DNA detection with pathology exaggerates risk and justifies indiscriminate testing and vaccination campaigns. If persistence were as common as claimed, millions of cancers would be expected annually. Instead, mortality continues to decline, driven by natural immunity, demographic transitions, and improved healthcare access.
Vaccine Efficacy: The Pointer–Eliminator Principle
The vaccine narrative collapses under both biological and epidemiological scrutiny. Vaccines and their dangerous antibodies function only as dangerous pointers, incapable of eliminating pathogens. True destruction is performed by immune effector mechanisms. Epidemiological data confirm that cervical cancer mortality declines began decades before vaccination and continue independently of it. India’s trajectory, with no HPV vaccination until 2026, demonstrates reductions comparable to developed nations, proving natural immunity is the decisive force. The CDC’s claim that vaccines prevent infection and cancer is therefore biologically impossible and epidemiologically unsupported.
Comparative Table: CDC Narratives vs HVBI Framework
Before presenting the table, it is important to emphasize that the CDC’s three claims—universality, persistence, and vaccine efficacy—are not neutral scientific statements but rhetorical devices designed to exaggerate risk and justify mass vaccination campaigns. The HVBI Framework systematically dismantles these presumptions by integrating clearance kinetics, stage‑specific progression timelines, and the Pointer–Eliminator Principle. The table below synthesizes these perspectives, contrasting CDC’s claims with biologically grounded realities.
Aspect
CDC Claim
HVBI Framework Evidence
Universality
HPV is “most common STI”
Only ~1% of population infected at any given time; >95% clear naturally within 2 years
Persistence
“Some infections persist and progress”
Of the 1% infected, 95% clear; remaining 5% → 4% clear at CIN1/2 stage; only ~1% of 5% of 1% persist (≈0.0005 of population)
Vaccine Efficacy
Vaccines prevent infection and cancer
Vaccines are dangerous pointers only; elimination is immune‑driven; declines predate vaccination
Analysis: From Biological Critique To Jurisprudential Remedy
The CDC’s rhetorical pillars collapse when confronted with biological plausibility and epidemiological data. Universality is disproven by the fact that only 1% of the population is infected at any given time, with nearly all clearing naturally. Persistence is dismantled by the vanishingly small fraction of infections that truly persist, amounting to 0.0005 of the population. Vaccine efficacy is refuted by the Pointer–Eliminator Principle and decades of declining cancer rates independent of vaccination.
Yet scientific critique alone is insufficient. Victims of HPV vaccine injuries remain without justice because immunity provisions shield corporations from accountability. Here, jurisprudential doctrines provide the necessary remedy. The Unacceptable Human Harm Theory (UHHT) asserts that no medical intervention should cause any harm, and when such harm occurs, immediate legal consequences must follow. UHHT strengthens the case for absolute liability, ensuring that accountability is not delayed or diluted by bureaucratic promises. The Oppressive Laws Annihilation (OLA) Theory confronts the reality that laws protecting corporations over human lives are instruments of tyranny. OLA demands ignoring of oppressive laws by people, dismantling of immunity provisions, and annulling legal shields that perpetuate systemic injustice. Together, UHHT and OLA provide a techno‑legal foundation for embedding absolute liability into U.S. law, ensuring that victims are no longer burdened with proving negligence and that accountability is automatic, enforceable, and uncompromising.
Conclusion
The CDC’s three pillars—universality, persistence, and vaccine efficacy—are unscientific, pseudoscientific, and disconnected from ground reality. HPV infections occur rarely and are overwhelmingly cleared naturally, persistence is vanishingly rare, and vaccines are biologically incapable of preventing infection or cancer. Epidemiological data confirm that cervical cancer incidence and mortality have been declining for decades, independent of vaccination, driven by natural immunity and healthcare improvements.
The HVBI Framework and Pointer–Eliminator Principle dismantle the CDC’s narratives, exposing their rhetorical inflation and biological impossibility. But critique must be matched with remedy. The doctrines of UHHT and OLA Theory provide that remedy, demanding absolute liability for HPV vaccines and the annulment of immunity provisions that shield corporations from accountability. Vaccine safety must not remain a matter of paper assurances—it must be a legally guaranteed right. Only by embedding absolute liability into U.S. law can justice be real, accountability be immediate, and human harm never tolerated.
Reject Hollow Assurances, Ditch HPV Death Shots, and Demand Absolute Liability for Medical Offenses in America.
The Centers for Disease Control and Prevention (CDC) has constructed its HPV vaccination campaign upon three rhetorical pillars: universality,persistence, and vaccine efficacy. Each claim, when examined through biological plausibility, epidemiological data, and immunological mechanisms, collapses under scrutiny. The HPV Vaccines Biological Impossibilities (HVBI) Framework and the Pointer–Eliminator Principle provide a coherent rebuttal, demonstrating that HPV infections are overwhelmingly transient, persistence is vanishingly rare, and vaccines are biologically incapable of preventing infection or cancer. Cervical cancer incidence and mortality have declined steadily for decades, independent of vaccination, driven by natural immunity, demographic transitions, and healthcare improvements. This article synthesizes the critiques of universality, persistence, and vaccine efficacy into a unified conclusion: the CDC’s narratives are pseudoscientific, misleading, and detrimental to evidence‑based public health, while the HVBI Framework restores scientific integrity and rational policy.
Introduction
HPV has been framed by the CDC as the “most common sexually transmitted infection,” with “some infections persisting and progressing to cancer,” and vaccines positioned as the decisive preventive tool. These claims, taken together, construct a narrative of inevitability: that nearly everyone is infected, many will persist, and vaccines are the only salvation. Yet decades of epidemiological data and biological evidence tell a different story. Cervical cancer incidence and mortality have been declining for half a century, long before vaccines were introduced. More than 95% of HPV infections clear naturally within 1–2 years, persistence occurs in fewer than 1% of cases at any given time, and progression to cancer is rarer still. Vaccines, operating only as pointers under the Pointer–Eliminator Principle, cannot prevent infection or cancer.
This introduction situates the CDC’s three claims within the broader pseudoscientific framework and sets the stage for a systematic synthesis. By integrating the HVBI Framework’s biological impossibilities with epidemiological trajectories, we demonstrate that universality, persistence, and vaccine efficacy are rhetorical inflations disconnected from ground reality.
Systematic Rebuttal Of CDC’s Pseudoscience By HVBI Framework
Universality
The CDC’s universality claim exaggerates risk by conflating transient viral DNA detection with persistent oncogenic disease. Transparent statistics show that more than 95% of infections clear naturally, undermining the presumption of inevitability. If the CDC’s backlog narrative were accurate, catastrophic cancer rates would be observed. Instead, SEER data confirm declining incidence and mortality independent of vaccination.
Persistence
The persistence narrative implies millions at risk of cancer, yet transparent statistics reveal persistence is vanishingly rare (<0.0005 of the population). Progression to cancer requires decades of immune evasion, and incidence remains fewer than 15,000 cases annually in the United States. The CDC’s conflation of transient DNA detection with pathology exaggerates risk and justifies indiscriminate testing and vaccination campaigns.
Vaccine Efficacy
The vaccine narrative collapses under the Pointer–Eliminator Principle. Vaccines and neutralizing antibodies function only as pointers, incapable of eliminating pathogens. True destruction is performed by immune effector mechanisms. Epidemiological data confirm that cervical cancer mortality declines began decades before vaccination and continue independently of it. India’s trajectory, with no vaccination until 2026, demonstrates reductions comparable to developed nations, proving natural immunity and healthcare improvements are the decisive forces.
Comparative Table: CDC Narratives vs HVBI Framework
Before presenting the table, it is important to emphasize that the CDC’s three claims — universality, persistence, and vaccine efficacy — are not neutral scientific statements but rhetorical devices designed to exaggerate risk and justify mass vaccination campaigns. The HVBI Framework systematically dismantles these presumptions by integrating clearance kinetics, stage‑specific progression timelines, and the Pointer–Eliminator Principle. The table below synthesizes these perspectives, contrasting CDC’s claims with biologically grounded realities.
Persistence <0.0005 of population; progression rarer still; incidence <15,000 annually
Vaccine Efficacy
Vaccines prevent infection and cancer
Vaccines are pointers only; elimination is immune‑driven; declines predate vaccination
The table demonstrates that CDC’s universality claim collapses under biological scrutiny. By labeling HPV as the “most common STI,” the CDC conflates transient viral DNA detection with persistent oncogenic disease, ignoring clearance kinetics and immune competence. The HVBI Framework reveals that more than 95% of infections resolve naturally, undermining the presumption of inevitability.
The persistence claim is equally dismantled. Transparent statistics show that persistence occurs in fewer than 0.0005 of the population, with progression rarer still. If persistence were as common as the CDC implies, millions of cancers would be expected annually. Instead, incidence remains fewer than 15,000 cases per year, with mortality declining steadily for decades, independent of vaccination.
The vaccine efficacy claim collapses under both biological and epidemiological scrutiny. Vaccines function only as pointers, incapable of eliminating pathogens. The Pointer–Eliminator Principle clarifies that destruction is performed exclusively by immune effector mechanisms. Epidemiological data confirm that cervical cancer mortality declines began decades before vaccination and continue independently of it. India’s trajectory, with no vaccination until 2026, demonstrates reductions comparable to developed nations, proving natural immunity and healthcare improvements are the decisive forces.
Together, the table underscores the superiority of the HVBI Framework over CDC’s rhetorical inflation. By juxtaposing CDC’s claims with biologically grounded realities, the disconnect between inflated narratives and actual disease burden becomes clear.
Conclusion
The CDC’s three pillars — universality, persistence, and vaccine efficacy — are unscientific, pseudoscientific, and disconnected from ground reality. Universality collapses under clearance kinetics, persistence is vanishingly rare, and vaccines are biologically incapable of preventing infection or cancer. Epidemiological data confirm that cervical cancer incidence and mortality have been declining for decades, independent of vaccination, driven by natural immunity, demographic transitions, and healthcare improvements.
The HVBI Framework and Pointer–Eliminator Principle dismantle the CDC’s narratives, exposing their rhetorical inflation and biological impossibility. Public health discourse must abandon fear‑based campaigns and instead embrace strategies grounded in biological plausibility, epidemiological evidence, and patient‑centered care. Only by respecting natural immunity, refining screening strategies, and improving healthcare access can cervical cancer elimination be achieved with integrity and scientific honesty.
On all three counts — universality, persistence, and vaccine efficacy — the CDC is wrong. On all three counts, the HVBI Framework is right.
Cervical cancer mortality has declined globally for decades, long before the introduction of HPV vaccines in 2006. Despite claims by the Centers for Disease Control and Prevention (CDC) that vaccines prevent infections leading to cancer, epidemiological evidence demonstrates that age‑standardized rates (ASR) and deaths were already falling due to natural immunity, demographic transitions, and healthcare improvements. India’s trajectory is particularly revealing: with negligible screening, poor treatment access, and no vaccination until 2026, India nonetheless achieved a 55% reduction in ASR and a 24% reduction in deaths between 1970 and 2026.
The HPV Vaccines Biological Impossibilities (HVBI) Theory, reinforced by the Pointer–Eliminator Principle formulated by Praveen Dalal, provides a conceptual framework for understanding why vaccines cannot prevent infection or cancer. The principle asserts that all targeting systems operate through two distinct stages: pointer (identification) and eliminator (destruction). Vaccines and neutralizing antibodies serve only as pointers, incapable of destroying pathogens. True elimination is performed by innate and adaptive immune effector mechanisms. This separation explains why vaccinated individuals remain susceptible to infection and progression, while natural immunity clears more than 90% of HPV infections without intervention.
By integrating epidemiological data, pharmacovigilance evidence, and the Pointer–Eliminator Principle, this article demonstrates that HPV vaccines have no measurable effect on preventing infection or cancer. The decline in cervical cancer mortality is independent of vaccination, and vaccine safety data are systematically underreported. The HVBI framework dismantles the CDC’s universality, persistence, and vaccine claims, restoring scientific integrity to public health discourse.
Introduction
Cervical cancer mortality has declined steadily across the globe for half a century. While HPV vaccination campaigns are often credited with this reduction, the evidence shows otherwise. Age‑standardized rates and deaths were already falling long before vaccines were introduced, driven primarily by natural immunity and gradual improvements in healthcare. India’s experience is particularly striking: despite negligible screening and treatment, and no vaccination until 2026, India achieved Death-To-Population Ratio (DPR) (mortality ratios) comparable to developed nations.
The HVBI Theory challenges the CDC’s three pillars of HPV rhetoric: universality, persistence, and vaccine efficacy. The first two have already been dismantled by epidemiological and biological evidence. This article focuses on the third pillar — the vaccine claim — and demonstrates its collapse through data analysis and conceptual critique. Central to this critique is the Pointer–Eliminator Principle, which clarifies why vaccines cannot prevent infection or cancer.
The Pointer–Eliminator Principle
Conceptual Foundation
The Pointer–Eliminator Principle asserts that all targeting systems operate through two sequential stages:
(1) Pointer (Identification): Marks the target but does not destroy it. (2) Eliminator (Destruction): Executes destruction based on the pointer’s signal.
In biological systems, vaccines and their antibodies are dangerous pointers. They may identify pathogens but cannot destroy them. The eliminator stage is performed by immune effector mechanisms such as macrophages, natural killer cells, cytotoxic T lymphocytes, and complement proteins.
Biological Illustration
(1) Strong Immune Systems: Innate immunity acts as both pointer and eliminator, clearing >90% of HPV infections naturally. (2) Weak Immune Systems: Vaccines provide artificial pointers, but elimination fails if innate immunity is compromised. (3) Vaccines Antibodies: They tag pathogens but do not kill them. Their role ends once identification is complete.
Technological Illustration
Photodynamic Therapy (PDT) mirrors the principle: a photosensitizer marks abnormal cells (pointer), while reactive oxygen species generated by light exposure destroy them (eliminator). This universality underscores the principle’s validity across disciplines.
Epidemiological Evidence Against Vaccine Efficacy
India’s Cervical Cancer Mortality Decline (1970–2026)
India provides one of the most compelling case studies for evaluating the true drivers of cervical cancer decline. Between 1970 and 2006, long before HPV vaccines were introduced, India experienced a steady reduction in both age‑standardized rates (ASR) and absolute deaths. This decline occurred despite negligible screening coverage (1–3%) and poor treatment access (1–2%). The reductions continued between 2006 and 2026, even though vaccination was not introduced nationally until 2026. These trends demonstrate that natural immunity and demographic changes, rather than vaccination, explain the decline.
Table 1: Cervical Cancer Mortality In India (1970–2026)
Year
ASR (per 100k)
Deaths (thousands)
Population (millions)
Deaths-to-Pop Ratio (%)
1970
~22
~55
555
0.0099%
2006
~14
~47
1,173
0.0040%
2026
~10
~42
1,476
0.0028%
The data confirm that India’s DPR/mortality ratio by 2026 (~0.0028%) is comparable to developed nations with decades of vaccination and screening. This outcome is achieved despite India’s minimal healthcare infrastructure and absence of vaccination until 2026. The evidence proves that vaccines cannot explain the decline. Instead, natural immunity, demographic transitions, and gradual improvements in healthcare are the decisive forces.
Global Comparison Of Cervical Cancer Mortality (1970–2026)
Global data reinforce the Indian case study. Countries such as the United States, United Kingdom, and Sweden show dramatic declines in cervical cancer mortality beginning in the 1970s, decades before HPV vaccines were introduced. These declines were driven by screening programs, improved treatment, and natural immunity. By comparing India with these nations, it becomes clear that vaccination is not the determining factor in reducing mortality.
Table 2: Global Decline In Cervical Cancer Mortality (1970–2026)
Country
1970 ASR/Deaths
2006 ASR/Deaths
2026 ASR/Deaths
Total Reduction (ASR/Deaths)
USA
~18 / ~15k
~6 / ~5k
~4 / ~3.5k
78% / 77%
UK
~20 / ~7k
~7 / ~2.5k
~5 / ~1.8k
75% / 74%
India
~22 / ~55k
~14 / ~47k
~10 / ~42k
55% / 24%
Global Avg
~20 / ~275k
~13 / ~180k
~9 / ~150k
55% / 45%
The global comparison demonstrates that declines in cervical cancer mortality are universal and began long before HPV vaccines. Cancer takes decades to develop, meaning vaccines introduced in 2006 could not plausibly reduce deaths by 2031-2036. The earliest measurable vaccine impact would be post 2031. Thus, attributing mortality reductions to vaccination is scientifically indefensible.
Pharmacovigilance Evidence Of Vaccine Pseudoscience
Beyond epidemiology, vaccine safety claims collapse under pharmacovigilance scrutiny. Passive surveillance systems such as VAERS, the Yellow Card Scheme, and EudraVigilance systematically underreport severe adverse events. The Oxford study (2025) revealed that fewer than 1% of severe events are reported, while the HVBI Framework (2026) validated this finding and established active surveillance as the benchmark.
Table 3: Underreporting Of Severe Adverse Events (Global Data)
Context
Estimated Reporting Rate
Key Evidence
Global Rates
~7%
Historical pharmacovigilance studies
Oxford Study
<1%
Cohort analysis, 2025
Canada
0%
Retrospective study, 2024
Nigeria
1,375 vs 34,000
WHO audit, 2016
Philippines
3 vs 12 per million
Regional data
The evidence confirms that vaccine safety data are systematically distorted. Severe adverse events such as hospitalization, disability, and death are rarely reported, undermining the CDC’s narrative of safety. The HVBI Framework demonstrates that passive systems are fundamentally inadequate, and vaccine safety claims rest on incomplete and manipulated data.
Biological Impossibility Of HPV Vaccine Cancer Prevention
The central flaw in the CDC’s vaccine narrative lies in its biological impossibility. Vaccines and the neutralizing antibodies they induce function only as pointers — they mark viral particles but do not destroy them. The Pointer–Eliminator Principle makes clear that destruction of pathogens is carried out exclusively by immune effector mechanisms such as macrophages, natural killer cells, cytotoxic T lymphocytes, and complement proteins. Since vaccines cannot perform the eliminator function, they cannot prevent HPV infections from occurring or persisting. If infection cannot be prevented, then the downstream progression to cancer cannot be interrupted by vaccination.
HPV infections are overwhelmingly transient, with more than 90% cleared naturally within two years by the innate and adaptive immune systems. Persistence occurs in fewer than 1% of cases at any given time, and progression to cancer is rarer still. Vaccines do not alter this natural clearance process; they merely tag viral particles without eliminating them. This means that vaccinated individuals remain fully susceptible to infection, persistence, and progression. The biological chain is straightforward: no infection prevention → no cancer prevention.
Epidemiological data reinforce this biological reality. Cervical cancer mortality has been declining globally for decades, long before HPV vaccines were introduced in 2006. India’s trajectory is especially revealing: despite negligible screening, poor treatment access, and no vaccination until 2026, India achieved reductions in age‑standardized rates and deaths comparable to developed nations. This proves that natural immunity and healthcare improvements, not vaccination, are the decisive forces behind cancer decline. Vaccines cannot be credited with reductions that began decades earlier and continued independently of their introduction.
Therefore, the CDC’s claim that HPV vaccines prevent cancer collapses under both biological and epidemiological scrutiny. Vaccines cannot prevent infection, and without infection prevention, cancer prevention is biologically impossible. The decline in cervical cancer mortality is driven by natural immunity, demographic transitions, and healthcare improvements. The eliminator is — and always has been — the human immune system. Vaccines, as mere pointers, are incapable of altering this reality.
Conclusion
The evidence presented in this article decisively proves that HPV vaccines have played no role in preventing HPV infections. More than 90% of infections are naturally cleared by the immune system within two years, and fewer than 1% persist at any given time. Vaccines, which function only as pointers under the Pointer–Eliminator Principle, cannot prevent infection because they do not destroy pathogens. Antibodies generated by vaccines merely tag viral particles; they do not kill them, neutralize them, or eliminate infected cells. The eliminator stage is performed exclusively by immune effector mechanisms, which operate independently of vaccination. Thus, the claim that vaccines prevent infection collapses under biological scrutiny.
If vaccines cannot prevent infection, they are biologically incapable of preventing cancer. Cervical cancer develops only after decades of persistent infection, a process that requires immune evasion and progression through precancerous stages. Since vaccines do not stop infections from occurring or persisting, they cannot interrupt the pathway to cancer. Epidemiological data confirm this: cervical cancer mortality has been declining steadily for decades, long before vaccines were introduced. India’s case study demonstrates that even without vaccination, DPR/mortality ratios fell to levels comparable with developed nations. This proves that natural immunity, demographic changes, and healthcare improvements — not vaccines — are the decisive forces behind cancer decline.
Pharmacovigilance evidence further dismantles the CDC’s vaccine narrative. Passive surveillance systems systematically underreport severe adverse events, with fewer than 1% of serious outcomes captured. The Oxford study (2025) and HVBI Framework (2026) validated this systemic underreporting, exposing the distorted foundation upon which vaccine safety claims rest. When severe adverse events such as hospitalization, disability, and death are omitted from the record, the narrative of vaccine safety becomes pseudoscientific. This distortion, combined with the biological impossibility of vaccines preventing infection, renders the CDC’s claim of cancer prevention indefensible.
Taken together, the universality claim, persistence claim, and vaccine claim collapse under the weight of epidemiological reality and biological logic. Vaccines cannot prevent infection, and therefore they cannot prevent cancer. The Pointer–Eliminator Principle clarifies why: vaccines are mere pointers, incapable of elimination. The eliminator is — and always has been — the human immune system. Public health discourse must therefore abandon fear‑based vaccine campaigns and instead focus on strengthening natural immunity, expanding screening, improving treatment access, and empowering communities. Only by respecting biological reality and epidemiological truth can cervical cancer elimination be achieved.
The Centers for Disease Control and Prevention (CDC) asserts that “some HPV infections can be persistent and can progress to cancer in both women and men later in life.” When coupled with the CDC’s universality claim, this statement creates a misleading narrative of inevitable oncogenic progression. By presuming that the majority of the population is infected, the CDC implies that millions are at risk of cancer. Yet epidemiological data, clearance kinetics, and immune‑stratified analyses reveal that persistent infections represent less than 1% of the population at any given time, and progression to cancer is rarer still.
This article demonstrates that the CDC’s persistence narrative is pseudoscientific, unprovable, and disconnected from ground reality. Using the HPV Vaccines Biological Impossibilities (HVBI) Framework, we show that persistence is rare, progression is exceptional, and cancer incidence continues to decline independent of vaccination. The persistence claim, like the universality claim, collapses under scrutiny.
Introduction
The CDC’s persistence narrative is not an isolated statement but a continuation of its universality rhetoric.If 90% of the population were truly infected, then “some” persisting would imply millions of ongoing oncogenic cases. Yet SEER data confirm fewer than 15,000 cervical cancer cases annually in the United States, a figure incompatible with CDC’s infection backlog. More than 95% of HPV infections clear naturally within 1–2 years, even for high‑risk strains such as HPV‑16 and HPV‑18. The persistence narrative conflates transient viral DNA detection with rare oncogenic progression, exaggerating risk and justifying mass vaccination campaigns. This introduction situates the persistence claim within the broader pseudoscientific framework and sets the stage for systematic rebuttal.
Epidemiological Disproof Of Persistence
The CDC’s persistence narrative collapses when contextualized against clearance kinetics and cancer incidence data. More than 95% of HPV infections resolve spontaneously within two years, even for high‑risk strains. If persistence were proportional to CDC’s inflated infection figures, catastrophic cancer rates would be observed. Instead, SEER data confirm declining incidence from 13.1 per 100,000 women in the mid‑1970s to 7.7 in 2022, with mortality dropping to 2.2 per 100,000.
At any given time, fewer than 1% of the population harbors persistent infection, undermining the CDC’s implication of widespread oncogenic risk. The persistence narrative therefore exaggerates risk by conflating transient viral DNA detection with rare oncogenic progression.
Natural History And Clinical Timelines
The natural history of HPV infection demonstrates that persistence and progression are strongly modulated by immune competence. In individuals with normal immune systems, infections are overwhelmingly transient and clinically insignificant. Weak immune systems show persistence, but CIN2/3 typically appears only after a decade, with cancer risk emerging after 25–30 years. Fast progressors and immunocompromised individuals face much shorter timelines, with CIN2/3 appearing within 5–10 years and invasive cancer within 10–15 years. Treatment outcomes vary: slow progressors respond well, while fast progressors and immunocompromised patients face higher recurrence risks.
Table 1: Consolidated Natural History, Progression, And Clinical Timelines (HPV‑16/18, Base Year: 2010)
Immune Category
Clearance / Persistence
CIN 2/3 Appearance
CIN 2/3 Duration
Invasive Cancer Timeline (No Treatment)
Time: Infection → AIS
Time: AIS → Cancer (No Treatment)
Screening at AIS Stage
Treatment at AIS Stage
Cancer Cases Despite Treatment (% of AIS)
Notes on Recurrence
Normal Immune System
>90% clear within 1–2 years
None
N/A
None
N/A
N/A
Not applicable
Not applicable
0%
Infection transient, clinically insignificant
Weak Immune System (Slow Progressors)
Partial control; high persistence
10–15 Years
10–15 Years
25–30 Years
~25 Years → 2035
~5 Years → 2040
Detectable at AIS (LEEP/cone usually curative)
High success; most cured
~5–10%
Recurrence usually occurs after 2040
Very Weak Immune System (Fast Progressors)
Poor control; rapid persistence
5–10 Years
~5 Years
10–15 Years
~15 Years → 2025
~5 Years → 2030
Detectable at AIS (requires aggressive excision)
Moderate success; higher recurrence risk
~15–20%
Recurrence can occur within or just beyond 2030
Immune‑Compromised (HIV / Severe Suppression)
Accelerated persistence
3–5 Years
<2 Years
5–10 Years
~7 Years → 2017
~3 Years → 2020
Detectable at AIS (needs strict monitoring)
Lower success; hysterectomy often required
~25–30%
Recurrence often rapid
Analysis:
This table demonstrates that persistence is not a universal phenomenon but a rare outcome tied to immune weakness. In normal immune systems, infections are transient and clinically insignificant, with no progression to CIN2/3 or cancer. Weak immune systems show persistence only after a decade, and even then, progression to invasive cancer requires 25–30 years. Fast progressors and immunocompromised individuals face shorter timelines, but these represent small subgroups of the population. Treatment outcomes vary, but even in high‑risk groups, recurrence rates remain limited. The data confirm that persistence is rare, progression rarer still, and cancer incidence is far below the catastrophic levels implied by CDC’s narrative.
Stage‑Based Testing Strategy
The CDC’s conflation of transient viral DNA detection with inevitable cancer progression is scientifically indefensible. A stage‑based analysis reveals that CIN1 and CIN2 often regress, while only CIN3 represents a true pre‑cancerous condition requiring intervention. Indiscriminate molecular testing exaggerates risk and leads to overtreatment, while targeted testing optimizes benefit‑harm balance.
Table 2: Stage‑Based Testing Strategy (HPV‑16/18)
Stage
Natural Course
Risk of Over‑Testing
Safe Testing / Intervention Window
Rationale
Initial Infection (HPV DNA+, no lesions)
≈95% clear within 1–2 years
Very high – most infections resolve naturally
Retest only if infection persists beyond 18–24 months
Early testing causes anxiety and overtreatment
CIN1 (low‑grade changes)
90% of persistent cases regress
High – regression is common
Repeat cytology/HPV testing in 12 months
Observation preferred
CIN2 (moderate changes)
Some regress, some progress
Moderate – depends on age and persistence
Monitor closely; treat if persistent
Balances regression potential with risk of progression
CIN3 (high‑grade changes)
Precancerous, unlikely to regress
Low – intervention justified
Immediate treatment (LEEP, conization)
True intervention point
AIS → Cancer
Rapid progression once AIS develops
N/A
Prevention relies on CIN3 detection
Detecting CIN3 early avoids progression
Analysis:
This table highlights the danger of indiscriminate molecular testing. At the initial infection stage, ≈95% of cases clear naturally, meaning early testing leads to unnecessary anxiety and overtreatment. CIN1 and CIN2 often regress, making observation the preferred strategy. Only CIN3 represents a true intervention point, where treatment is justified and effective. AIS progresses rapidly to cancer, but prevention relies on detecting CIN3 early. The HVBI Framework demonstrates that targeted, stage‑based testing achieves superior benefit‑harm balance compared to universal molecular screening, dismantling the CDC’s persistence narrative.
Comparative Analysis Of CDC Persistence Claim vs HVBI Framework
The persistence narrative can be directly contrasted with the HVBI Framework. While the CDC frames persistence as a significant threat, the HVBI Framework demonstrates that persistence is rare, progression rarer still, and cancer incidence continues to decline. Transparent statistics show that only 1% of the population is infected at a given time, 95% of these clear naturally, 4% regress at CIN1/CIN2, and only 1% of 5% of 1% progress beyond CIN3/AIS.This translates to less than 0.0005 of the total population — a vanishingly rare outcome.
Table 3: Comparative Analysis Of CDC Persistence Claim vs HVBI Framework
Aspect
CDC Claim
HVBI Framework Evidence
Persistence
“Some infections persist and progress”
Transparent statistics show only 1% of the population is infected at a given time. Of this 1%, 95% clear naturally, 4% regress at CIN1/CIN2, and only 1% of 5% of 1% progress beyond CIN3/AIS. Persistence is therefore <0.0005 of the total population — vanishingly rare.
Cancer Risk
Implied millions at risk
Actual burden is fewer than 15,000 cervical cancer cases annually in the U.S.; incidence and mortality have been declining for decades, independent of vaccination.
Biological Basis
DNA detection conflated with pathology
Clearance kinetics show >95% of infections resolve naturally; persistence requires rare immune evasion and does not equate to cancer.
Screening Strategy
Universal molecular testing
Targeted immune‑stratified approach: PCR/genotyping reserved for persistent infections beyond clearance windows, older individuals with concerning cytology, and immunocompromised patients.
Analysis Of Table 3
This comparative table exposes the fundamental weakness in the CDC’s persistence narrative. By stating that “some infections persist and progress,” the CDC implies a significant public health burden. Yet transparent statistics reveal that only 1% of the population is infected at any given time, and of this small fraction, 95% clear the infection naturally. The remaining 5% are not destined for cancer; 4% regress at CIN1 and CIN2 stages, leaving only 1% of 5% of 1% — less than 0.0005 of the total population — progressing beyond CIN3/AIS.This vanishingly small risk dismantles the CDC’s suggestion of widespread persistence and progression.
The cancer risk narrative is equally misleading. If persistence were as common as the CDC implies, millions of cancers would be expected annually. Instead, SEER data confirm fewer than 15,000 cervical cancer cases per year in the United States, with incidence and mortality declining steadily for decades, independent of vaccination. The biological basis of the CDC’s claim is flawed, as it conflates transient DNA detection with pathology. More than 95% of infections resolve naturally, and persistence requires rare immune evasion. Screening strategies further highlight the disconnect: universal molecular testing exaggerates risk and leads to overtreatment, while targeted immune‑stratified approaches achieve superior benefit‑harm balance. Together, these analyses confirm that the CDC’s persistence claim is pseudoscience, disconnected from biological and epidemiological reality.
Broader Implications Of The Persistence Narrative
The CDC’s persistence claim is not simply a scientific statement; it functions as a rhetorical device that exaggerates risk and justifies mass vaccination campaigns. By presenting persistence as a common outcome, the CDC implies that millions of individuals are at risk of cancer, despite epidemiological data showing otherwise. This narrative conflates transient viral DNA detection with pathology, ignoring the biological reality that more than 95% of infections resolve naturally. The transparent statistics demonstrate that persistence is vanishingly rare, occurring in less than 0.0005 of the total population. Such a small risk cannot justify the sweeping generalizations and fear‑based messaging embedded in the CDC’s persistence claim.
The persistence narrative also undermines rational public health policy. By exaggerating risk, it encourages indiscriminate molecular testing and mass vaccination strategies that yield minimal benefit and substantial harms and deaths. Over‑testing leads to anxiety, unnecessary procedures, and overtreatment, while mass vaccination campaigns are justified on the basis of inflated infection and persistence figures. In contrast, the HVBI Framework demonstrates that targeted, immune‑stratified screening strategies achieve superior benefit‑harm balance, focusing resources on high‑risk individuals while avoiding unnecessary interventions in the vast majority of the population.
Conclusion
First, the CDC’s claim that some HPV infections persist and progress to cancer is not an epidemiological fact but a rhetorical device designed to exaggerate risk and justify mass vaccination campaigns. Transparent statistics reveal that only 1% of the population is infected at a given time, 95% of these clear naturally, 4% regress at CIN1/CIN2, and only 1% of 5% of 1% progress beyond CIN3/AIS. Persistence is therefore vanishingly rare, occurring in less than 0.0005 of the total population.
Second, the CDC’s persistence narrative collapses when contextualized against clearance kinetics and cancer incidence data. If persistence were proportional to CDC’s inflated infection figures, catastrophic cancer rates would be observed. Instead, SEER data confirm fewer than 15,000 cervical cancer cases annually in the United States, with incidence and mortality declining steadily for decades, independent of vaccination.
Third, the CDC’s conflation of transient viral DNA detection with inevitable pathology is scientifically indefensible. Stage‑based testing reveals that only CIN3 represents the decisive intervention point, and inflated persistence figures risk fear‑based messaging and unnecessary interventions. The HVBI Framework provides a biologically grounded progression model that dismantles the CDC’s persistence narrative.
Finally, immune‑stratified screening strategies demonstrate the superiority of targeted PCR/genotyping over indiscriminate molecular testing. Routine early testing yields minimal benefit and substantial harms, while targeted testing optimizes benefit‑harm balance. Implementing immune‑informed PCR triage reduces unnecessary procedures, concentrates resources on high‑risk individuals, and supports patient‑centered, evidence‑based screening policies.
In light of these analyses, the CDC’s persistence claim is unscientific, pseudoscientific, and disconnected from ground reality—just as its universality claim was. Together, these narratives form a foundation of pseudoscience that must be dismantled to restore integrity to public health discourse and to promote rational, evidence‑based strategies that respect biological reality and epidemiological truth.
India’s case is particularly compelling and is a global scientific and epidemiological example that can never be rebutted by the HPV pseudoscience and pharma cartel. Despite negligible screening, poor treatment coverage, and no HPV vaccination until 2026, the country has achieved mortality reductions comparable to high-income nations. The introduction of the Death-to-Population Ratio (DPR) as the ninth stage of HVBI Frameowrk provides a revolutionary metric that contextualizes mortality relative to population size, exposing the distortion of fear-driven narratives.
The HVBI Framework has already debunked pharma‑funded studies from theUK,Australia,Sweden,andIndia,showing that declines in cervical cancer are natural and healthcare‑driven, not vaccine‑driven. More debunked bogus studies are in pipeline.
HPV vaccines have been aggressively promoted worldwide as the cornerstone of cervical cancer prevention. Yet, the scientific foundations of these claims are riddled with assumptions: that microabrasions are ubiquitous gateways, that infection is near-universal, that natural clearance is dangerous, and that vaccines alone explain cancer declines. The HVBI Framework, developed through rigorous analysis, has systematically dismantled these assumptions across eight stages. Now, with the addition of DPR as the ninth stage, HVBI integrates demographic science into its critique, providing a holistic epidemiological and ethical rebuttal.
India’s trajectory is central to this global debate. Between 1970 and 2026, India achieved a 55% reduction in age-standardized rates (ASR) and a 24% reduction in deaths, despite minimal screening and treatment infrastructure. Most strikingly, India’s DPR in 2026 (~0.0028%) is comparable to Japan and Italy, nations with decades of screening and vaccination programs. This unrebuttable scientific and epidemiological proof reveals the resilience of natural immunity and the distortion inherent in vaccine-centric narratives. By contextualizing India’s progress, HVBI exposes the pseudoscience of HPV vaccines and reframes cervical cancer prevention around evidence-based proportional risk.
Natural History And Clinical Timelines
Table 1: Consolidated Natural History, Progression, And Clinical Timelines (HPV‑16/18, Base Year: 2010)
Immune Category
Clearance / Persistence
CIN 2/3 Appearance
CIN 2/3 Duration
Invasive Cancer Timeline (No Treatment)
Time: Infection → AIS
Time: AIS → Cancer (No Treatment)
Screening at AIS Stage
Treatment at AIS Stage
Cancer Cases Despite Treatment (% of AIS)
Notes on Recurrence
Normal Immune System
>90% clear within 1–2 years
None
N/A
None
N/A
N/A
Not applicable
Not applicable
0%
Infection transient, clinically insignificant
Weak Immune System (Slow Progressors)
Partial control; high persistence
10–15 Years
10–15 Years
25–30 Years
~25 Years → 2035
~5 Years → 2040
Detectable at AIS (LEEP/cone usually curative)
High success; most cured
~5–10%
Recurrence usually occurs after 2040
Very Weak Immune System (Fast Progressors)
Poor control; rapid persistence
5–10 Years
~5 Years
10–15 Years
~15 Years → 2025
~5 Years → 2030
Detectable at AIS (requires aggressive excision)
Moderate success; higher recurrence risk
~15–20%
Recurrence can occur within or just beyond 2030
Immune‑Compromised (HIV / Severe Suppression)
Accelerated persistence
3–5 Years
<2 Years
5–10 Years
~7 Years → 2017
~3 Years → 2020
Detectable at AIS (needs strict monitoring)
Lower success; hysterectomy often required
~25–30%
Recurrence often rapid
Analysis: In normal immune systems, infections are transient and clinically insignificant. Weak immune systems show persistence, with CIN2/3 appearing after a decade and cancer risk emerging only after 25–30 years. Fast progressors and immunocompromised individuals face much shorter timelines, with CIN2/3 appearing within 5–10 years and invasive cancer within 10–15 years. Treatment outcomes vary: slow progressors respond well, while fast progressors and immunocompromised patients face higher recurrence risks.
Stage-Based Testing Strategy
Table 2: Stage‑Based Testing Strategy (HPV‑16/18)
Stage
Natural Course
Risk of Over‑Testing
Safe Testing / Intervention Window
Rationale
Initial Infection (HPV DNA+, no lesions)
≈95% clear within 1–2 years
Very high – most infections resolve naturally
Retest only if infection persists beyond 18–24 months
Early testing causes anxiety and overtreatment
CIN1 (low‑grade changes)
90% of persistent cases regress
High – regression is common
Repeat cytology/HPV testing in 12 months
Observation preferred
CIN2 (moderate changes)
Some regress, some progress
Moderate – depends on age and persistence
Monitor closely; treat if persistent
Balances regression potential with risk of progression
CIN3 (high‑grade changes)
Precancerous, unlikely to regress
Low – intervention justified
Immediate treatment (LEEP, conization)
True intervention point
AIS → Cancer
Rapid progression once AIS develops
N/A
Prevention relies on CIN3 detection
Detecting CIN3 early avoids progression
Analysis: At the initial infection stage, most cases clear naturally within two years, so retesting is only warranted if persistence lasts beyond 18–24 months. CIN1 and CIN2 are transitional stages where regression is common, especially in younger women, making observation and repeat testing the safest approach. CIN3, however, represents the decisive intervention point, as lesions are precancerous and unlikely to regress. Immediate treatment at this stage prevents progression to AIS and invasive cancer.
Cervical Cancer Mortality In India
Table 3: Cervical Cancer Mortality In India (1970–2026)
Year
ASR (per 100,000 women)
Deaths (thousands)
Population (millions)
Deaths-to-Population Ratio (%)
1970
~22
~55
555
0.0099%
1980
~20
~53
698
0.0076%
1990
~18
~50
873
0.0057%
2000
~16
~48
1,058
0.0045%
2006
~14
~47
1,173
0.0040%
2010
~13
~46
1,243
0.0037%
2020
~11
~45
1,403
0.0032%
2026
~10
~42
1,476
0.0028%
Analysis: India’s deaths-to-population ratio by 2026 (~0.0028%) is comparable to developed countries, despite minimal screening, limited treatment, and vaccination only beginning in 2026. Indians survived HPV from 1970 to 2026 only on the basis of the natural immune system.
Global Comparison
Table 4: Global Comparison: 1970–2026
Rank
Country
1970 (ASR / Deaths k)
2006 (ASR / Deaths k)
% Reduction 1970–2006 (ASR / Deaths)
2026 (ASR / Deaths k)
% Reduction 2006–2026 (ASR / Deaths)
Total Reduction 1970–2026 (ASR / Deaths)
Pop. 2026 (m)
Deaths-to-Pop Ratio 2026 (%)
1
United States
~18 / ~15
~6 / ~5
67% / 67%
~4 / ~3.5
33% / 30%
78% / 77%
340
0.0010%
2
United Kingdom
~20 / ~7
~7 / ~2.5
65% / 64%
~5 / ~1.8
29% / 28%
75% / 74%
68
0.0026%
3
Sweden
~17 / ~1.5
~6 / ~0.5
65% / 67%
~4 / ~0.3
33% / 40%
76% / 80%
10
0.0030%
4
Canada
~18 / ~2.5
~7 / ~1
61% / 60%
~5 / ~0.7
29% / 30%
72% / 72%
39
0.0018%
5
Australia
~19 / ~2
~8 / ~0.8
58% / 60%
~5 / ~0.6
38% / 25%
74% / 70%
26
0.0023%
6
France
~21 / ~6
~9 / ~2.5
57% / 58%
~6 / ~1.8
33% / 28%
71% / 70%
68
0.0026%
7
Germany
~20 / ~7
~9 / ~3
55% / 57%
~6 / ~2.1
33% / 30%
70% / 70%
84
0.0025%
8
Japan
~17 / ~10
~8 / ~4.5
53% / 55%
~6 / ~3.5
25% / 22%
65% / 65%
123
0.0028%
9
Italy
~19 / ~5
~9 / ~2.3
53% / 54%
~6 / ~1.6
33% / 30%
68% / 68%
60
0.0027%
10
Spain
~18 / ~4
~9 / ~2
50% / 50%
~6 / ~1.4
33% / 30%
67% / 65%
47
0.0030%
11
India
~22 / ~55
~14 / ~47
36% / 15%
~10 / ~42
29% / 11%
55% / 24%
1,476
0.0028%
12
Global Avg
~20 / ~275
~13 / ~180
35% / 35%
~9 / ~150
31% / 17%
55% / 45%
8,000
0.0019%
Analysis: This comparison demonstrates that India’s proportional risk, measured through DPR, is now equivalent to many high-income nations despite negligible screening, poor treatment, and nil vaccination until 2026. The declines in ASR and deaths in India mirror global averages, proving that natural immunity and demographic resilience are sufficient to achieve parity. The data also shows that vaccines cannot explain declines before 2026, as cervical cancer takes decades to develop and measurable vaccine impact would only appear around 2045–2050. India’s case dismantles the global pseudoscientific narrative that vaccines are the sole drivers of progress.
Conventional metrics exaggerate India’s cervical cancer burden by focusing on raw deaths
DPR contextualizes mortality relative to population, showing India’s risk is comparable to developed nations
Reframes cervical cancer discourse: India’s proportional risk is low, progress is real, and coercive HPV vaccination campaigns are unjustified
Analysis: The HVBI Framework provides a comprehensive dismantling of pseudoscientific assumptions surrounding HPV infections and HPV vaccines. Stages 1–6 challenge the biological foundations of mainstream claims, showing that infection is not universal, natural clearance is safe and effective, and vaccines act more as “dangerous alarms” than shields. Stage 7 expands the critique into epidemiology, exposing how long-term declines in HPV-related cancers are misattributed to vaccines despite evidence that these trends predate vaccination programs. Stage 8 escalates the framework into the ethical domain, framing coercive vaccine promotion as medical genocide when severe adverse effects are ignored and natural immunity data suppressed. Stage 9 completes the framework by introducing DPR, a quantitative metric that contextualizes mortality relative to population size. This reframing dismantles fear-driven narratives and proves that India’s proportional risk is comparable to developed nations, despite nil screening, treatment, and HPV vaccination until 2026.
Conclusion
The HVBI Framework, now expanded to nine stages with DPR, provides an irrefutable scientific and ethical rebuttal to HPV vaccine pseudoscience. India’s trajectory proves that natural immunity, demographic resilience, and stage-based screening are sufficient to achieve parity with developed nations. DPR contextualizes mortality, dismantling fear-driven narratives and exposing the manipulation of raw death counts. Together, the HVBI Framework and DPR make the vaccine-centric narrative scientifically untenable and ethically indefensible. The evidence is overwhelming: cervical cancer declines are natural, healthcare-driven, and demographic in nature, not vaccine-driven.
This article establishes that the future of cervical cancer prevention lies not in coercive vaccination but in transparent, evidence-based strategies that respect natural immunity and proportional risk. The case is closed: HPV pseudoscience has been decisively rebutted, and the HVBI Framework makes it impossible to argue otherwise.
The Centers for Disease Control and Prevention (CDC) continues to assert that “Human papillomavirus (HPV) is the most common sexually transmitted infection in the United States.” This sweeping claim has been used as a rhetorical foundation for mass vaccination campaigns, yet it collapses under scrutiny when examined through biological, epidemiological, and immunological evidence. Drawing upon four critical analyses—(1) the HVBI Framework’s rebuttal of universality, (2) statistical and epidemiological disproof of CDC’s infection backlog narrative, (3) stage‑based testing and burden analysis, and (4) immune‑stratified natural history and screening strategy—this article synthesizes evidence to demonstrate that the CDC’s claim is unscientific, unprovable, and misleading. The data reveal that HPV infections are overwhelmingly transient, that cervical cancer incidence and mortality have declined independent of vaccination, and that targeted screening strategies yield superior benefit‑harm balance compared to indiscriminate molecular testing. By integrating these perspectives, this article concludes that the CDC’s universality narrative is pseudoscience, unsupported by ground reality, and detrimental to evidence‑based public health.
Introduction
The CDC’s framing of HPV as the “most common sexually transmitted infection” is not a neutral epidemiological statement but a rhetorical device designed to exaggerate risk and justify widespread vaccination programs as proved by CDC Is Pushing Unscientific And Unproven HPV Vaccine Pseudoscience: HVBI Framework. Within the HPV Vaccines Biological Impossibilities (HVBI) Framework (HVBI Framework), this presumption of universality violates biological plausibility and conflates transient viral DNA detection with persistent oncogenic disease. The claim of 42 million current infections and 13 million new annual infections, if taken literally, would imply catastrophic cancer rates that are not observed. Instead, decades of epidemiological data confirm declining cervical cancer incidence and mortality, driven by natural immunity and screening, not vaccination. This introduction situates the CDC’s claim within the broader context of pseudoscientific narratives and sets the stage for a systematic rebuttal.
Epidemiological Disproof Of Universality
The CDC’s figures—42 million infections and 13 million new annual cases—are biologically impossible when contextualized against clearance kinetics and cancer incidence data as proved by The Unprovable And Untraceable HPV Infection Pseudoscience Of CDC. More than 95% of HPV infections clear spontaneously within two years, even for high‑risk strains such as HPV‑16 and HPV‑18. If the CDC’s backlog narrative were accurate, the United States would face hundreds of thousands of cervical cancers annually. Instead, SEER data confirm a decline in incidence from 13.1 per 100,000 women in the mid‑1970s to 7.7 in 2022, with mortality dropping to 2.2 per 100,000. These declines occurred despite population growth and before HPV vaccination was introduced, underscoring the role of natural immunity and screening.
Stage‑Based Testing And Burden Analysis
The CDC’s conflation of transient viral DNA detection with inevitable pathology is scientifically indefensible as proved by HPV Infection Burden And Stage‑Based Testing. More than 95% of infections resolve naturally, and only a small minority persist long enough to progress through CIN3, AIS, and invasive cancer. If the CDC’s figures represented persistent oncogenic disease, catastrophic cancer rates would be observed. Instead, epidemiological evidence confirms declining incidence and mortality. The HPV Vaccines Biological Impossibilities (HVBI) Framework (HVBI Framework) demonstrates that infection counts must be contextualized within clearance kinetics and stage‑specific timelines, which show that only CIN3 represents the decisive intervention point. Inflated infection numbers risk fear‑based messaging and unnecessary interventions.
Immune‑Stratified Screening Strategy
HPV’s natural history is strongly modulated by host immune competence, with ≈95% of infections clearing within 1–2 years as outlined in Immune‑Stratified Natural History And Screening Strategy. Routine early molecular testing in immunocompetent populations yields minimal benefit and substantial harms through over‑testing and overtreatment. A targeted strategy—reserving PCR/genotyping for persistent infections beyond clearance windows, older individuals with concerning cytology, and immunocompromised patients—achieves superior benefit‑harm balance. This immune‑stratified approach aligns biological timelines with pragmatic screening thresholds, discouraging premature intervention and promoting judicious, evidence‑based management.
Table: Comparative Analysis Of CDC Claims And HVBI Framework
Before presenting the table, it is important to emphasize that the CDC’s universality narrative rests on presumptions rather than direct epidemiological evidence. The HVBI Framework systematically dismantles these presumptions by integrating clearance kinetics, stage‑specific progression timelines, and immune‑stratified screening strategies. The table below synthesizes these perspectives, contrasting CDC’s rhetorical inflation with biologically grounded realities.
The table is not merely a summary but a critical tool for understanding how inflated infection counts collapse under scrutiny. By juxtaposing CDC’s claims with HVBI’s evidence, the table reveals the disconnect between raw infection numbers and actual disease burden, highlighting the superiority of targeted, immune‑stratified approaches over indiscriminate molecular testing.
Biologically impossible without catastrophic cancer rates
Epidemiology
Justifies mass vaccination
SEER data show declining incidence/mortality independent of vaccination
Stage‑Based Testing
Conflates DNA detection with pathology
Only CIN3 is decisive intervention point
Screening Strategy
Early molecular testing for all
Targeted PCR/genotyping for persistent, high‑risk, or immunocompromised
Analysis Of Table
The table demonstrates that CDC’s universality claim is a rhetorical inflation unsupported by biological or epidemiological evidence. By labeling HPV as the “most common STI,” the CDC conflates transient viral DNA detection with persistent oncogenic disease, ignoring clearance kinetics and immune competence. The HVBI Framework reveals that more than 95% of infections resolve naturally, undermining the presumption of inevitability.
The infection burden figures—42 million current infections and 13 million new annually—are biologically impossible when contextualized against cancer incidence data. If these figures represented persistent oncogenic disease, catastrophic cancer rates would be observed. Instead, SEER data confirm declining incidence and mortality, driven by natural immunity and screening, not vaccination. This disconnect exposes the CDC’s narrative as pseudoscience.
Finally, the table underscores the superiority of targeted, immune‑stratified screening strategies over indiscriminate molecular testing. Routine early PCR/genotyping yields minimal benefit and substantial harms, while targeted testing optimizes benefit‑harm balance. The HVBI Framework provides a biologically grounded, evidence‑based approach that dismantles CDC’s universality narrative and promotes rational public health policy.
Conclusion
First, the CDC’s claim that HPV is the most common sexually transmitted infection in the United States is not an epidemiological fact but a rhetorical device designed to exaggerate risk and justify mass vaccination campaigns. The HVBI Framework demonstrates that this presumption of universality collapses under scrutiny, as transient infections dominate and more than 95% clear naturally.
Second, the CDC’s infection burden figures—42 million current infections and 13 million new annually—are biologically impossible when contextualized against clearance kinetics and cancer incidence data. If these figures represented persistent oncogenic disease, catastrophic cancer rates would be observed. Instead, SEER data confirm declining incidence and mortality, independent of vaccination, driven by natural immunity and screening.
Third, the CDC’s conflation of transient viral DNA detection with inevitable pathology is scientifically indefensible. Stage‑based testing reveals that only CIN3 represents the decisive intervention point, and inflated infection numbers risk fear‑based messaging and unnecessary interventions. The HVBI Framework provides a biologically grounded progression model that dismantles CDC’s backlog narrative.
Finally, immune‑stratified screening strategies demonstrate the superiority of targeted PCR/genotyping over indiscriminate molecular testing. Routine early testing yields minimal benefit and substantial harms, while targeted testing optimizes benefit‑harm balance. Implementing immune‑informed PCR triage reduces unnecessary procedures, concentrates resources on high‑risk individuals, and supports patient‑centered, evidence‑based screening policies.
In light of these analyses, the CDC’s universality claim is unscientific, pseudoscientific, and disconnected from ground reality.
Human papillomavirus (HPV), particularly oncogenic types 16 and 18, follows a heterogeneous natural history strongly modulated by host immune competence. Global population data (1970–2026) indicate a steady-state point prevalence of ≈1% infected at any time, with ≈95% of those infections clearing within 1–2 years and ≈5% persisting; of that persistent 5% only a small fraction progress to high‑grade disease (CIN3, AIS) and invasive cancer. Using the timelines and parameters of HPV Vaccines Biological Impossibilities (HVBI) Framework, and synthesizing successive analyses provided earlier, this article presents an immune‑category framework (Normal, Weak/Slow Progressors, Very Weak/Fast Progressors, Immune‑Compromised) that aligns biological timelines with pragmatic PCR testing thresholds and clinical action points. We reproduce four foundational tables detailing progression and treatment timelines and add a fifth table proposing PCR‑triage thresholds matched to immune status and observed epidemiologic fractions. For each table we offer interpretive analyses that integrate prevalence, clearance, progression probabilities, and recurrence risk. We conclude that routine early molecular genotyping or immediate intervention at first detection in largely immunocompetent populations results in substantial over‑testing and potential over‑treatment; instead, targeted delayed molecular triage based on persistence, age, cytologic change, or immunocompromise optimizes benefit‑harm balance and resource allocation.
Introduction
HPV types 16 and 18 are principal drivers of cervical intraepithelial neoplasia (CIN), adenocarcinoma in situ (AIS), and invasive cervical cancer. However, the majority of HPV infections are transient and clinically silent; immune response is the chief determinant of clearance versus persistence. Public‑health policy and clinical practice must therefore reconcile the small absolute risk of progression for most individuals with the need to identify and treat the minority at real risk for high‑grade disease. Misaligned screening—testing or treating too early—creates harms through anxiety, overtreatment, morbidity from unnecessary procedures, and inefficient use of limited diagnostic resources.
This paper synthesizes a sequence of analyses into a coherent, evidence‑informed model that: (1) reproduces established progression timelines stratified by immune competence; (2) maps those timelines onto screening and treatment decision thresholds; (3) provides explicit PCR/genotyping triage recommendations to minimize over‑testing; and (4) argues against premature population‑wide molecular testing and intervention absent persistence or high‑risk clinical markers. The tables that follow are intended as operational tools for clinicians and policymakers to align screening frequency and molecular triage with biological risk.
Tables For Global Population-Level Studies, Analysis And Stats For HPV-16 And HPV-18
The four foundational tables reproduced below encapsulate consolidated natural history, treatment reset dynamics, CIN3 progression timelines, and an age‑specific case study for a cohort infected in 2010, stratified by immune competence. These tables integrate the supplied global prevalence parameters (1% point prevalence, 95% clearance in 1–2 years, 5% persistence among the 1%, with only ~1% of that persistent pool progressing to CIN3/AIS/cancer) and the stage‑based clinical framework used to guide intervention thresholds.
Following the foundational tables, a fifth table is added that operationalizes PCR/genotyping thresholds tied to immune category, persistence intervals, cytologic findings, and age—designed to guide clinicians away from premature testing and toward targeted, high‑yield molecular triage. Each table is followed by analysis that integrate timeline, prevalence, and clinical implications, culminating in a conclusion that argues for restraint in initiating molecular testing or invasive treatment before biologically plausible windows for progression have elapsed.
Table 1: Consolidated Natural History, Progression, And Clinical Timelines (HPV‑16/18, Base Year: 2010)
Immune Category
Clearance / Persistence
CIN 2/3 Appearance
CIN 2/3 Duration
Invasive Cancer Timeline (No Treatment)
Time: Infection → AIS
Time: AIS → Cancer (No Treatment)
Screening at AIS Stage
Treatment at AIS Stage
Cancer Cases Despite Treatment (% of AIS)
Notes on Recurrence
Normal Immune System
>90–95% clear within 1–2 years; after clearance no downstream disease
None
N/A
None
N/A
N/A
Not applicable
Not applicable
0%
Infection transient, clinically insignificant
Weak Immune System (Slow Progressors)
Partial control; persistent pool ≈5% of the 1% infected
10–15 Years
10–15 Years
25–30 Years
~25 Years → 2035
~5 Years → 2040
Detectable at AIS (LEEP/cone usually curative)
High success; most cured
~5–10%
Recurrence usually occurs after 2040, often outside AIS→Cancer window
Very Weak Immune System (Fast Progressors)
Poor control; rapid persistence; part of small persistent fraction
5–10 Years
~5 Years
10–15 Years
~15 Years → 2025
~5 Years → 2030
Detectable at AIS (may require aggressive excision)
Moderate success; higher recurrence risk
~15–20%
Recurrence can occur within or just beyond 2030, limiting long‑term benefit
Recurrence often rapid, sometimes within AIS→Cancer window; treatment durability reduced
Analysis
Table 1 emphasizes the central role of immune competence in shaping HPV‑16/18 natural history. In those with normal immune function, the near‑universal clearance within 1–2 years effectively eliminates downstream risk for CIN1/2/3, AIS, and invasive cancer; these individuals constitute the majority of the infected pool and account for negligible clinical disease. In contrast, the small persistent pool (≈5% of the 1% infected) contains the individuals who may progress to high‑grade disease. Weak (slow) progressors have protracted timelines that afford generous windows for observation and intervention, while very weak and immunocompromised groups display compressed timelines that demand earlier detection and more aggressive management.
Clinically, the table supports differential screening intensity: population‑level programs should avoid immediate genotyping at first detection for the immunocompetent majority, instead relying on observation and repeat testing at defined persistence intervals. Conversely, for those identified as fast progressors or immune‑compromised, earlier molecular confirmation and expedited diagnostic pathways are justified to prevent progression during shortened biological windows and to mitigate higher recurrence risk post‑treatment.
Table 2: Treatment Reset Timelines (HPV‑16/18)
Immune Category
Natural AIS→Cancer Window
Recurrence Timeline After Treatment
Interpretation
Weak (Slow Progressors)
2035 → 2040
2045–2050 or later
Treatment resets the clock; failures are technical/medical, not immune‑biological.
Very Weak (Fast Progressors)
2025 → 2030
2030–2035
Treatment buys time but recurrence may still occur within or just beyond the natural window.
Immunocompromised
2017 → 2020
2020–2023
Treatment does not reset the clock; recurrence is rapid and often within the natural window.
Analysis
Table 2 frames treatment as a temporal reset mechanism whose durability varies by immune status. In slow progressors, local excisional therapies (e.g., LEEP/cone) commonly achieve long disease‑free intervals, effectively postponing progression beyond the natural AIS→cancer window. This supports a conservative surveillance posture with high expectations for curative intent when CIN3/AIS is treated.
For fast progressors, treatment confers only a moderate time gain; recurrences may still fall within the expected natural window, necessitating closer post‑treatment surveillance. In immunocompromised patients, therapy often fails to confer durable protection—recurrence is both earlier and more frequent—underscoring the need for intensified monitoring and the limited value of aggressive early screening in the absence of clear high‑risk markers (beyond acknowledging that these patients do need early and frequent evaluation).
Table 3: CIN3 Progression Timelines (HPV‑16/18, Base Year: 2010)
Immune Category
Time: Infection → CIN3
Time: CIN3 → AIS
Notes on Progression
Weak Immune System (Slow Progressors)
~20 Years → 2030
~5 Years → 2035
CIN3 appears around 2030; if untreated, progresses to AIS by 2035. Treatment at CIN3 stage is often curative, with high regression potential.
Very Weak Immune System (Fast Progressors)
~10 Years → 2020
~5 Years → 2025
CIN3 appears much earlier, around 2020; progresses to AIS by 2025. Treatment at CIN3 stage reduces risk but recurrence can occur within the natural window.
Immune‑Compromised (HIV / Severe Suppression)
~5 Years → 2015
~2 Years → 2017
CIN3 appears rapidly, by 2015; progresses to AIS by 2017. Treatment at CIN3 stage is less effective, recurrence is frequent and aggressive.
Analysis
Table 3 positions CIN3 as the critical intervention point prior to AIS. For slow progressors, the long latency to CIN3 (≈20 years) creates a wide opportunity for detection at a time when treatment is highly effective. This large window reduces the urgency for early molecular genotyping at initial detection in low‑risk individuals.
The shortened timelines in fast progressors and immunocompromised patients compress the opportunity for detection, making earlier or more frequent surveillance reasonable. However, even in these groups, targeting molecular diagnostics to those with persistent HPV or cytologic change remains preferable to universal early genotyping, which would capture many transient infections without improving outcomes.
Table 4: Case Study – Ideal CIN3 Testing Timeline For A Girl Aged 13 In 2010 (HPV‑16/18)
Immune Category
Natural CIN3 Onset (Base Year 2010)
Biologically Impossible Before
Ideal Testing Window for CIN3
Rationale
Normal Immune System
No CIN3 (infection clears)
CIN3 progression biologically impossible
Not applicable
>90–95% clearance; transient infection.
Weak Immune System (Slow Progressors)
~2030 (she is 33 years old)
Before ~2025 (age 28) biologically impossible
2028–2030
CIN3 appears only after ~20 years; testing just before onset ensures detection.
Very Weak Immune System (Fast Progressors)
~2020 (she is 23 years old)
Before ~2018 (age 21) biologically impossible
2018–2020
CIN3 onset ~10 years post‑infection; testing captures early progression.
Immunocompromised (HIV / Severe Suppression)
~2015 (she is 18 years old)
Before ~2014 (age 17) biologically impossible
2014–2015
CIN3 onset ~5 years post‑infection; testing must occur very early.
Analysis
Table 4 translates generalized timelines into age‑anchored testing windows for an illustrative cohort. It highlights that biologic plausibility constrains the earliest ages at which CIN3 can reasonably be expected to appear. Screening prior to those windows primarily detects transient infections and risks overdiagnosis.
For public‑health programs, the case study reinforces age‑ and risk‑tailored policies: defer aggressive molecular/genotypic screening in the general adolescent and young adult population, while ensuring early testing pathways for immunocompromised youth or those with persistent abnormal cytology.
Table 5: PCR/Triage Thresholds By Immune Competence (HPV‑16/18, Base Year: 2010)
Immune Category
Clearance / Persistence
PCR/Triage Trigger (Stage)
Recommended Interval to PCR after CIN (based on CIN→AIS window)
Action if Positive
Notes on Recurrence
Normal Immune System
>90–95% clear within 1–2 years; after clearance no downstream disease
None required
N/A
None required
Infection transient, clinically insignificant
Weak Immune System (Slow Progressors)
Persistent pool ≈5% of the 1% infected
CIN3 stage
~5 years (CIN3 → AIS window)
Genotype → colposcopy/biopsy if 16/18 positive or cytology ≥CIN3; treat per guidelines
Recurrence usually after 2040, often outside AIS→Cancer window
Very Weak Immune System (Fast Progressors)
Rapid persistence within small fraction
CIN2 stage (progresses rapidly to CIN3)
~5 years (CIN2/CIN3 → AIS window)
Immediate colposcopy/biopsy if 16/18 or cytology ≥CIN2; expedited treatment
~2–3 years (CIN1/CIN3 → AIS window) or immediate at HPV+
Urgent colposcopy/biopsy and early treatment; intensified follow‑up post‑treatment
Recurrence often rapid, sometimes within AIS→Cancer window
Analysis
Table 5 emphasizes that PCR/genotyping should be strategically timed to the CIN→AIS progression window, which represents the last safe checkpoint before invasive potential emerges. Up to CIN3, clearance remains possible — with spontaneous regression documented even at high‑grade lesions. Therefore, premature molecular testing during the natural clearance phase (first 2 years post‑infection, or early CIN stages) risks over‑diagnosis and unnecessary intervention. By anchoring PCR to the CIN→AIS window, testing is reserved for the point where clearance has demonstrably failed and progression risk becomes clinically significant.
Clinically, this approach balances vigilance with restraint. For weak progressors, PCR is deferred until CIN3, exploiting the long latency and high regression potential. For very weak progressors, PCR is advanced to CIN2, reflecting their compressed timelines. In immune‑compromised individuals, the CIN→AIS window is so short that PCR must be triggered at CIN1 or even the first HPV+ detection. This tiered strategy ensures that molecular confirmation is withheld in the transient majority but accelerated in biologically vulnerable subgroups, aligning testing intensity with true progression risk.
Conclusion
The presented synthesis—grounded in prevalence figures and immune‑stratified timelines of HVBI Framework—reaffirms that immune competence is the primary determinant of clinically meaningful HPV‑16/18 disease. The overwhelming majority of infections are transient; therefore, routine early PCR genotyping or immediate intervention at first detection in the general, immunocompetent population yields minimal clinical benefit and substantial harms through over‑testing and overtreatment.
Instead, a targeted strategy that reserves PCR/genotyping for (a) persistent infections beyond biologically plausible clearance windows, (b) older individuals or those with concerning cytology, and (c) immunocompromised patients, achieves superior benefit‑harm balance.
Implementing immune‑informed PCR triage reduces unnecessary procedures, concentrates clinical resources on the small high‑risk fraction who actually progress to CIN3/AIS/cancer, and supports patient‑centered, evidence‑based screening policies. The data and tables herein provide a practical operational framework to discourage premature screening/testing/treatment and to promote judicious, biology‑aligned clinical management.
The Centers for Disease Control and Prevention (CDC) asserts that more than 42 million Americans are currently infected with disease‑associated human papillomavirus (HPV) types, with approximately 13 million new infections occurring annually. These figures are presented as evidence of a widespread, persistent threat, justifying aggressive vaccination campaigns. However, such claims are not based on direct testing data but on presumptions that conflate transient viral DNA detection with clinically significant disease. Rigorous biological analysis demonstrates that over 95% of HPV infections, including high‑risk oncogenic types such as HPV‑16 and HPV‑18, clear spontaneously within two years in immunocompetent individuals. Only a small minority persist long enough to progress through the multi‑decade sequence of cervical intraepithelial neoplasia grade 3 (CIN3), adenocarcinoma in situ (AIS), and invasive cervical cancer.
Cross‑referencing CDC prevalence claims with Surveillance, Epidemiology, and End Results (SEER) program data reveals a sustained decline in cervical cancer incidence and mortality in the United States since the mid‑1970s, driven by natural immunity, Pap screening, and treatment of precancers—not HPV vaccination. If the CDC’s backlog of 42 million infections and 13 million new annual cases represented persistent oncogenic disease, the U.S. would face hundreds of thousands of cervical cancers annually, a scenario contradicted by observed epidemiology (~13,490 cases and ~2,100 deaths yearly). This article integrates stage‑specific progression tables, case studies, and treatment outcomes to demonstrate that the CDC’s framing is scientifically unsound. The conclusion is clear: the CDC’s infection counts are rhetorical inflation, not epidemiological reality.
Introduction
HPV is a ubiquitous virus, but ubiquity does not equate to inevitability of disease. The CDC’s claim of 42 million current infections and 13 million new infections annually positions HPV as a near‑universal, persistent threat. Yet, these figures reflect transient viral DNA detection rather than clinically significant persistence. More than 95% of infections resolve naturally, and only a small minority progress to CIN3 and beyond.
Historical and contemporary epidemiological data confirm this disconnect. Cervical cancer incidence has declined by more than 50% since the mid‑1970s, despite population growth. Mortality has dropped to 2.2 per 100,000 women in 2022. These declines occurred before and independent of HPV vaccination, introduced in 2006. The biological impossibility of the CDC’s backlog claim becomes evident when progression timelines are considered: infection to CIN3 takes 5–20 years, and CIN3 to cancer takes 3–15 years untreated. If tens of millions of persistent infections existed, the U.S. would face catastrophic cancer rates, which is not observed.
Natural History, Progression, And Treatment Outcomes
Understanding the natural history of HPV‑16/18 infections is essential before evaluating claims of widespread persistent disease. The majority of infections, even those caused by high‑risk oncogenic strains, are transient and clear spontaneously within one to two years in immunocompetent individuals. Only a small minority persist, and among these, progression to precancerous lesions such as CIN2/3 and eventually invasive cancer takes place over decades. This slow trajectory underscores that infection alone does not equate to disease, and that immune strength plays a decisive role in determining whether HPV remains clinically insignificant or evolves into a serious condition.
Treatment outcomes further highlight the importance of immune status and stage of detection. While early lesions (CIN1 and CIN2) often regress naturally, CIN3 represents the true intervention point where treatment is both necessary and effective. At this stage, procedures such as LEEP or conization can prevent progression to AIS and invasive cancer. However, recurrence risks vary: slow progressors benefit most, with recurrences occurring outside the natural AIS→Cancer window, while fast progressors and immunocompromised individuals face higher recurrence rates within the natural progression timeline. These dynamics make clear that stage‑based testing and intervention, rather than indiscriminate screening or inflated infection counts, provide the most rational and scientifically grounded approach to HPV management.
Table 1: Consolidated Natural History, Progression, And Clinical Timelines (HPV‑16/18, Base Year: 2010)
Immune Category
Clearance / Persistence
CIN 2/3 Appearance
CIN 2/3 Duration
Invasive Cancer Timeline (No Treatment)
Time: Infection → AIS
Time: AIS → Cancer (No Treatment)
Screening at AIS Stage
Treatment at AIS Stage
Cancer Cases Despite Treatment (% of AIS)
Notes on Recurrence
Normal Immune System
>90% clear within 1–2 years
None
N/A
None
N/A
N/A
Not applicable
Not applicable
0%
Infection transient, clinically insignificant
Weak Immune System (Slow Progressors)
Partial control; high persistence
10–15 Years
10–15 Years
25–30 Years
~25 Years → 2035
~5 Years → 2040
Detectable at AIS (LEEP/cone usually curative)
High success; most cured
~5–10%
Recurrence usually occurs after 2040, outside AIS→Cancer window
Very Weak Immune System (Fast Progressors)
Poor control; rapid persistence
5–10 Years
~5 Years
10–15 Years
~15 Years → 2025
~5 Years → 2030
Detectable at AIS (requires aggressive excision)
Moderate success; higher recurrence risk
~15–20%
Recurrence can occur within or just beyond 2030, limiting benefit
Immune‑Compromised (HIV / Severe Suppression)
Accelerated persistence
3–5 Years
<2 Years
5–10 Years
~7 Years → 2017
~3 Years → 2020
Detectable at AIS (needs strict monitoring)
Lower success; hysterectomy often required
~25–30%
Recurrence often rapid, sometimes within AIS→Cancer window
Analysis:
This table highlights how immune strength dictates HPV‑16/18 progression. In normal immune systems, infections are transient and clinically insignificant. Weak immune systems show persistence, with CIN2/3 appearing after a decade and cancer risk emerging only after 25–30 years. Fast progressors and immunocompromised individuals face much shorter timelines, with CIN2/3 appearing within 5–10 years and invasive cancer within 10–15 years. Treatment outcomes vary: slow progressors respond well, while fast progressors and immunocompromised patients face higher recurrence risks, often within the natural AIS→Cancer window.
Table 2: Treatment Reset Timelines (HPV‑16/18)
Immune Category
Natural AIS→Cancer Window
Recurrence Timeline After Treatment
Interpretation
Weak (Slow Progressors)
2035 → 2040
2045–2050 or later
Treatment resets the clock; failures are technical/medical, not immune system based/biological.
Very Weak (Fast Progressors)
2025 → 2030
2030–2035
Treatment buys time but recurrence may still occur within or just beyond the natural window.
Immunocompromised
2017 → 2020
2020–2023
Treatment does not reset the clock; recurrence is rapid and often within the natural window.
Analysis:
This table shows how treatment interacts with natural progression. For slow progressors, treatment is highly effective, essentially resetting the biological clock and delaying recurrence for decades. Fast progressors benefit less, as recurrence often occurs within or just beyond the natural AIS→Cancer window. Immunocompromised patients gain the least benefit, with recurrence rapid and often within the natural window, underscoring the limited durability of treatment in this group.
Table 3: CIN3 Progression Timelines (HPV‑16/18, Base Year: 2010)
Immune Category
Time: Infection → CIN3
Time: CIN3 → AIS
Notes on Progression
Weak Immune System (Slow Progressors)
~20 Years → 2030
~5 Years → 2035
CIN3 appears around 2030; if untreated, progresses to AIS by 2035. Treatment at CIN3 stage is often curative, with high regression potential.
Very Weak Immune System (Fast Progressors)
~10 Years → 2020
~5 Years → 2025
CIN3 appears much earlier, around 2020; progresses to AIS by 2025. Treatment at CIN3 stage reduces risk but recurrence can occur within the natural window.
Immune‑Compromised (HIV / Severe Suppression)
~5 Years → 2015
~2 Years → 2017
CIN3 appears rapidly, by 2015; progresses to AIS by 2017. Treatment at CIN3 stage is less effective, recurrence is frequent and aggressive.
Analysis:
CIN3 is the last reliable intervention point before AIS. Slow progressors reach CIN3 after about 20 years, offering a long detection window and high regression potential if treated. Fast progressors reach CIN3 within 10 years, and immunocompromised patients within 5 years, both progressing quickly to AIS. Treatment at CIN3 is less effective in these groups, with frequent recurrence. This emphasizes the need for earlier and more frequent screening in high‑risk populations.
Table 4: Case Study – Ideal CIN3 Testing Timeline For A Girl Aged 13 In 2010 (HPV‑16/18)
Immune Category
Natural CIN3 Onset (Base Year 2010)
Biologically Impossible Before
Ideal Testing Window for CIN3
Rationale
Normal Immune System
No CIN3 (infection clears)
CIN3 progression biologically impossible
Not applicable
>90% clearance; transient infection.
Weak Immune System (Slow Progressors)
~2030 (she is 33 years old)
Before ~2025 (age 28) biologically impossible
2028–2030
CIN3 appears only after ~20 years; testing just before onset ensures detection.
Very Weak Immune System (Fast Progressors)
~2020 (she is 23 years old)
Before ~2018 (age 21) biologically impossible
2018–2020
CIN3 onset ~10 years post‑infection; testing captures early progression.
Immunocompromised (HIV / Severe Suppression)
~2015 (she is 18 years old)
Before ~2014 (age 17) biologically impossible
2014–2015
CIN3 onset ~5 years post‑infection; testing must occur very early.
Analysis:
This case study translates the general timelines of HPV‑16/18 progression into a practical scenario, showing how immune strength and age interact to determine when CIN3 becomes biologically possible. For individuals with normal immune systems, CIN3 never develops, making testing unnecessary. In contrast, slow progressors reach CIN3 only after about 20 years, meaning the earliest biologically possible onset is around age 28, with the ideal testing window between ages 28–30. Fast progressors and immunocompromised individuals face much shorter timelines, with CIN3 appearing by ages 23 and 18 respectively, requiring testing windows as early as 17–20 years of age.
The critical clarification here is that testing before the biologically possible onset is futile and risks overdiagnosis. Table 4 emphasizes that CIN3 cannot appear before certain ages depending on immune strength, so premature screening would only detect transient infections. By aligning testing windows with biological reality, the case study ensures that screening is both efficient and meaningful. This avoids unnecessary interventions in those who will clear the infection naturally, while still capturing progression in the small subset at risk.
Table 5: Stage‑Based Testing Strategy (HPV‑16/18)
Stage
Natural Course
Risk of Over‑Testing
Safe Testing / Intervention Window
Rationale
Initial Infection (HPV DNA+, no lesions)
≈95% clear within 1–2 years
Very high – most infections resolve naturally
Retest only if infection persists beyond 18–24 months
Early testing causes anxiety and overtreatment; persistence beyond 2 years signals risk group (≈5%).
CIN1 (low‑grade changes)
90% of persistent cases regress
High – regression is common
Repeat cytology/HPV testing in 12 months
Observation preferred; aggressive treatment unnecessary at this stage.
CIN2 (moderate changes)
Some regress, some progress
Moderate – depends on age and persistence
Monitor closely; treat if persistent (esp. in older women)
Balances regression potential with risk of progression; individualized approach.
CIN3 (high‑grade changes)
Precancerous, unlikely to regress
Low – intervention justified
Immediate treatment (LEEP, conization)
True intervention point; prevents progression to AIS and invasive cancer.
AIS → Cancer
Rapid progression once AIS develops
N/A – testing too late
Prevention relies on CIN3 detection
Detecting CIN3 early avoids reaching AIS/cancer stage.
Analysis:
This table outlines a general clinical framework for stage‑based testing, focusing on minimizing overtreatment while ensuring timely intervention. At the initial infection stage, most cases clear naturally within two years, so retesting is only warranted if persistence lasts beyond 18–24 months. CIN1 and CIN2 are transitional stages where regression is common, especially in younger women, making observation and repeat testing the safest approach. CIN3, however, represents the decisive intervention point, as lesions are precancerous and unlikely to regress. Immediate treatment at this stage prevents progression to AIS and invasive cancer.
The clarification here is that Table 5 provides broad rules applicable to all populations, while Table 4 contextualizes these rules with age‑specific timelines. Together, they eliminate ambiguity: testing should not occur prematurely at the infection or CIN1 stage, but should be timed to capture CIN3 onset, which varies by immune strength. This ensures that resources are directed toward the 5% of persistent cases, avoiding unnecessary interventions in the 95% who clear naturally. The strategy is therefore consistent across both tables—stage‑based testing is the guiding principle, with CIN3 as the critical checkpoint for intervention.
Discussion
The CDC’s claim of 42 million infections and 13 million new annual cases conflates transient viral DNA detection with persistent oncogenic disease. The biological progression framework demonstrates that only a small minority of infections persist long enough to matter clinically. If the CDC’s figures represented persistent disease, cervical cancer incidence would be orders of magnitude higher than observed. Instead, SEER data confirm declining incidence and mortality, driven by natural clearance and screening.
The HPV Vaccines Biological Impossibilities (HVBI) Framework (HVBI Framework) clarifies that infection counts are rhetorical inflation. Just as PCR detection of rhinoviruses or coronaviruses does not justify mass vaccination against the common cold, detection of transient HPV DNA does not justify fear‑based vaccine mandates. The analogy underscores the pseudoscientific nature of conflating viral presence with inevitable pathology.
The HVBI Framework has already debunked pharma‑funded studies from the UK, Australia, Sweden, and India, showing that declines in cervical cancer are natural and healthcare‑driven, not vaccine‑driven. More debunked bogus studies are in pipeline.
Conclusion
The CDC’s assertion of 42 million current HPV infections and 13 million new annual infections is not only misleading but scientifically indefensible when examined against the natural history of HPV, stage‑specific progression data, and decades of epidemiological evidence. More than 95% of HPV infections clear spontaneously within two years, even for high‑risk oncogenic strains such as HPV‑16 and HPV‑18. Only a small minority persist long enough to progress through the multi‑decade sequence of CIN3, AIS, and invasive cancer. If the CDC’s figures truly represented persistent oncogenic disease, the United States would be experiencing hundreds of thousands of cervical cancer cases annually. Instead, SEER data confirm that incidence has declined by more than 50% since the mid‑1970s, and mortality has dropped to 2.2 per 100,000 women in 2022. These declines occurred despite population growth and before HPV vaccination was introduced, driven overwhelmingly by natural immunity, Pap screening, and treatment of precancers.
The conclusion is therefore unavoidable: the CDC’s backlog narrative is a rhetorical inflation that conflates transient viral DNA detection with inevitable pathology. It is biologically impossible for 42 million persistent infections and 13 million new persistent cases per year to exist without catastrophic cancer rates, which are not observed. The HVBI Framework demonstrates that infection counts must be contextualized within clearance kinetics and stage‑specific timelines, which show that only CIN3 represents the decisive intervention point. Policy built on inflated infection numbers risks fear‑based messaging and unnecessary medical interventions, rather than evidence‑based prevention. Transparent communication of clearance rates, the effectiveness of screening, and the limited proportion of infections that persist is the only scientifically valid approach. In light of the data, the CDC’s claims are not just exaggerated—they are unscientific presumptions that collapse under scrutiny, leaving no room for rebuttal.
The Centers for Disease Control and Prevention (CDC) maintains that more than 42 million Americans are currently infected with disease-associated human papillomavirus (HPV) types, with approximately 13 million new infections occurring annually. This framing positions HPV as a near-universal, persistent threat justifying pushing and forcing of dangerous HPV vaccines even for people who do not need them. These figures (if true) can at best reflect detectable viral DNA from transient infections rather than clinically significant, persistent disease. Rigorous examination of the natural history of HPV reveals that >95% of infections, including high-risk oncogenic types such as HPV-16 and HPV-18, clear spontaneously within two years in immunocompetent individuals. Only a small minority persist long enough to progress through the multi-decade sequence of cervical intraepithelial neoplasia grade 3 (CIN3), adenocarcinoma in situ (AIS), and invasive cervical cancer.
Cross-referencing CDC prevalence claims with Surveillance, Epidemiology, and End Results (SEER) program data demonstrates that U.S. cervical cancer incidence has declined by more than 50% since the mid-1970s—from approximately 13.1 per 100,000 women in 1973–1975 to 7.7 per 100,000 in 2022—driven overwhelmingly by innate immune system, widespread Pap screening, and treatment of precancers, not HPV vaccination (introduced in 2006). The mortality rate (ASMR) also decline to 2.2 in 2022.
Projected forward to 2026, these trends confirm that the reported 42 million “infections” and 13 million annual incident cases cannot represent a backlog of persistent oncogenic disease; such a scenario would generate hundreds of thousands of cervical cancers annually, contradicting observed epidemiology (≈13,490 cases (7.5) and 2,100 deaths (2.1) yearly).
The U.S. resident population on July 1, 1975 was 215,465,000 (215.465 million) and U.S. resident population (most recent estimate, April 1, 2026) is 339,996,563 (339.997 million). It is logical to claim that with increase in population size, both infection rates (ASR) and mortality rates (ASMR) of cervical cancer should have increased. But this did not happen. On the contrary, both ASR and ASMR dropped upto 3/4th times (75%) in US. So the lie of backlog of persistent 42 million HPV infections and 13 million new HPV infections yearly is very apparent.
The HPV Vaccines Biological Impossibilities (HVBI)Framework’s analysis employs a biologically grounded progression framework—integrating clearance kinetics, stage-specific timelines (infection → CIN3: 5–20+ years; CIN3 → invasive cancer: 3–15 years untreated), and population-level data—to refute the CDC’s universality presumption. Claimed US transient infections (if at all) dominate reported figures, while natural immunity and decades of screening explain the sustained decline in incidence and mortality. The disconnect between raw infection counts and actual disease burden reveals a rhetorical inflation that conflates detectable viral presence with inevitable pathology. Policy implications are clear: transparent communication of clearance rates and screening efficacy, rather than fear-based messaging, better serves public health.
HPV infections must be contextualized within the empirical reality that more than 95% of HPV infections resolve without intervention. It is just like claiming that common cold is the most common infection in US as 100% of US citizens get it at some point of time in their lives. Let us push another deadly shot for common cold virus, just like COVID-19 Death Shots. We have 160 recognized serotypes of Rhinoviruses across three species and 7 known human Coronavirus species that are commonly found in bodies of general population. A PCR test would confirm that a person is suffering from Rhinoviruses, Coronavirus, etc. Would this justify forcing of Death Shots upon poulation? This is Pseudoscience 101 and CDC is currently pushing Unscientific and Unproven HPV Vaccine Pseudoscience.
Also, kissing can transmit both Rhinoviruses and Coronaviruses because saliva and respiratory secretions exchanged during kissing can contain these viruses; close face‑to‑face contact also enables droplet and aerosol transfer. Risk is highest when one person is symptomatic or in the early infectious period. Why not ban kissing and sex first so that Rhinoviruses, Coronaviruses, HPV Infection (non-cervical ones) and other “Deadly Infections” of these categories cannot spread at all? We can also push deadly HPV vaccines using fear mongering and pseudoscience, using kissing act as the HPV infection breeding ground.
Introduction
Public health messaging on human papillomavirus (HPV) has long centered on its status as “the most common sexually transmitted infection” in the United States, supported by CDC estimates of 42 million prevalent disease-associated infections and 13 million new cases annually. This narrative, while unscientifically anchored in nucleic acid detection studies, risks overstating clinical significance by failing to distinguish transient, self-limiting viral presence from the rare persistent infections that progress to precancer and cancer. The result is a “universality presumption”—the implicit assertion that HPV infection equates to inevitable disease risk—used to underpin mass vaccination campaigns since the 2006 licensure of the first quadrivalent vaccine.
Yet epidemiological reality tells a different story. Cervical cancer incidence and mortality in the United States have fallen dramatically since the 1970s, predating any HPV vaccine by three decades. By 2026 (estimated), age-adjusted incidence stands at 7.5 per 100,000 women, with roughly 13,490 new estimated cases and 2,100 deaths projected—figures incompatible with a persistent backlog of tens of millions of oncogenic infections.
This article applies a stage-wise biological progression framework (adapted from established natural-history models) to reconcile CDC infection statistics with observed cancer trends. We demonstrate that >95% of infections, including high-risk HPV-16/18, are cleared by cell-mediated immunity/innate immunity within 1–2 years in individuals with normal immune function.
Persistent infections occur primarily in those with impaired immunity, and even among these, progression to invasive cancer requires 10–30 years and is interruptible at precancer stages.
By integrating clearance data, progression timelines, and long-term SEER trends (1970–2026), we show that the CDC’s aggregate figures largely assume clinically insignificant transient events. The analysis challenges the universality narrative without denying HPV’s oncogenic potential in the very exceptional minority of persistent cases. Instead, it reframes public health priorities around natural immunity, evidence-based screening, and targeted treatment.
Natural History And Clearance Kinetics Of HPV Infection
The biological course of HPV infection is well-characterized: most genital infections are asymptomatic and resolve without sequelae. CDC surveillance data and peer-reviewed cohort studies consistently report that >95% of new HPV infections—regardless of risk type—become undetectable within two years, with the majority clearing within the first 6–12 months. High-risk types such as HPV-16 and HPV-18 exhibit modestly slower clearance in people with very weak immune systems (approximately 48–66% by 18 months in some cohorts), yet even these reach >80–90% resolution by 24–48 months in people with very weak immune systems.
Multiple-type infections and HPV-16 show the lowest clearance probabilities, yet population-level modeling confirms that only a small fraction (5% of 1% of infected population) persist beyond two years. Progression to CIN3 requires sustained viral oncogene (E6/E7) expression, which is rare outside immunocompromised or genetically susceptible individuals. Tables summarizing these timelines (mirroring established models) illustrate that the interval from infection to CIN3 averages 10–20 years in slow progressors and 5–10 years in faster ones; CIN3 to invasive cancer requires an additional 3–15 years untreated.
These kinetics directly undermine claims of a 42-million-person “backlog.” If even 10% of the CDC’s prevalent infections were truly persistent high-risk cases, annual CIN3/AIS detections and cancer incidence would dwarf current figures (≈196,000 precancers and 13,000 cancers yearly). Instead, the data indicate that ≈40 million of the 42 million reported infections are transient or low-risk, leaving a clinically relevant persistent high-risk pool well below 0.5–1 million at any time.
CDC Infection Statistics Versus Observed Disease Burden
The CDC’s 42 million prevalence and 13 million incidence figures derive from nucleic acid testing in nationally representative surveys and transmission-dynamic models. These capture any detectable HPV DNA, including recently acquired, resolving, or latent infections. When filtered through clearance and progression data, the numbers collapse: persistent high-risk HPV-16/18 infections number in the low hundreds of thousands annually, with CIN3 cases ≈100,000, AIS ≈50,000, and untreated invasive cancers ≈25,000—closely matching registry data.
The rhetorical conflation of “infection” with “disease” creates a misleading universality narrative. Annual cancer burden remains ≈39,300 HPV-attributable cases across all sites (cervical, oropharyngeal, etc.), representing <0.1% of the 13 million new infections. This mismatch is biologically expected, not anomalous.
Population-Level Trends In Cervical Cancer Incidence And Mortality (1970–2026)
SEER and CDC data document a >50% decline in cervical cancer incidence from the mid-1970s peak (≈13–18 per 100,000) to current levels (7.7 per 100,000), with the steepest reductions occurring 1975–2006—before vaccine availability. Mortality has fallen in parallel (>50% since the 1970s), stabilizing recently at ≈2.2 per 100,000 (in 2022, 2.1 in 2026). Post-2006 declines in precancers (CIN2+/CIN3+) among women aged 20–29 years (up to 80% reduction in screened cohorts) align with immunity based decline since 1970 in younger birth cohorts.
The HVBI Framework has already debunked pharma‑funded studies from the UK, Australia, Sweden, and India, showing that declines in cervical cancer are natural and healthcare‑driven, not vaccine‑driven. More debunked bogus studies are in pipeline.
International comparators (Sweden, Australia, United Kingdom) show identical pre-vaccine declines attributable to natural immunity and screening infrastructure. The U.S. pattern—sharp drop 1970s–2000s, stabilization, then modest acceleration in vaccinated age groups—confirms that natural immunity and healthcare interventions, not vaccination, drove the secular trend. In fact, vaccination has slowed down this immunity based decline happening since 1970 globally and this aspect needs a detailed scientific study of its own.
Implications For Public Health Policy And The Limits Of Universality Rhetoric
The biological and epidemiological record demonstrates that untraceable and unprovable transient infections dominate CDC statistics, while natural immunity and screening have rendered cervical cancer largely preventable for decades.
Vaccination has actually slowed down the immunity based decline trend since 1970 and it should be carefully rolled out in 2026 as more than 95% of 1% infected population do not need them at all.
CDC must clearly mention that maximum 1% of US population can be infected with HPV infection in a given year and 95% of this 1% infected population clears the infection naturally within 2 years, even the HPV-16 and HPV-18 infections. Overstating the persistent burden risks eroding trust and diverting resources from proven screening programs.
Conclusion
The CDC’s presentation of 42 million prevalent and 13 million annual HPV infections, is not even technically accurate for detectable DNA and it fundamentally misrepresents the clinical landscape when viewed through the lens of natural clearance kinetics and long-term cancer trends. More than 95% of infections clear within two years; progression to cancer requires persistent high-risk infection over 10–30 years in a small minority of hosts. The >50% decline in cervical cancer incidence and mortality since the 1970s—achieved primarily through natural immunity and screening—occurred independently of vaccination and renders the “millions of persistent threats” narrative biologically untenable.
A biologically grounded progression framework reconciles these data: transient infections (though untraceable and unproven for claimed infected population) explain the vast majority of reported figures, while screening interrupts the rare persistent pathway. Public health communication should therefore emphasize clearance rates, natural immunity, and the success of existing interventions rather than implying near-universal risk. Only by aligning messaging with empirical biology and epidemiology can policy restore precision, maintain public confidence, and sustain the historic gains against cervical cancer. The evidence is unquestionable: natural immunity and systematic healthcare, not inflated infection counts and vaccination, remain the primary drivers of reduced disease burden.
The Centers for Disease Control and Prevention (CDC) begins its HPV vaccine safety page with the sweeping assertion: “Human papillomavirus (HPV) is the most common sexually transmitted infection in the United States” (CDC HPV vaccine safety page). This statement is not a neutral epidemiological fact but a rhetorical device designed to exaggerate risk, instill fear, and justify mass vaccination campaigns. Within the HVBI Stage-Wise Framework, this claim directly violates the Near-Universal Infection Presumption critique and indirectly touches upon the Microabrasions Presumption.
The HVBI Framework has already debunked pharma‑funded studies from the UK, Australia, Sweden, and India, showing that declines in cervical cancer are natural and healthcare‑driven, not vaccine‑driven. More debunked bogus studies are in pipeline.
But CDC was still plagued with the pharma-controlled Advisory Committee on Immunization Practices (ACIP), that not only caused problems for US citizens but also for global stakeholders. With the constitution of new ACIP in 2025, CDC started taking corrective actions but the ACIP was dragged into a court case by AAP. The District Court granted a temporary stay and gave an opportunity to remove all procedural irregularities in the constitution and appointment of 2025 ACIP. Although the 2025 ACIP ensured Pluralistic Expertise In Vaccine Policy, yet its procedural irregularities created temporary problems. The renewal of 2025 ACIP tenure and formulation of a New ACIP Charter corrected those procedural defects.
CDC’s Narrative Of Universality
Despite this, the website of CDC is still pushing Unscientific and Unproven HPV Vaccine Pseudoscience as of 13-04-2026. By labeling HPV as “the most common sexually transmitted infection,” the CDC implies inevitability: that virtually all sexually active individuals will contract HPV. This narrative sustains the presumption of universality. Such framing was central to the CDC’s justification for widespread vaccination programs, but it collapses under HVBI’s systematic critique.
The HVBI Stage-Wise Framework provides a comprehensive systematic dismantling of the pseudoscientific assumptions surrounding HPV vaccines by progressing through eight stages of critique. In Stages 1–6, HVBI challenges the biological foundations of mainstream HPV vaccine claims, showing that infection is not universal, natural clearance is safe and effective, and vaccines act more as alarms than shields. It further demonstrates that vaccines are over-credited for cancer reduction, while the true drivers—natural clearance and screening—are consistently undervalued.
Stage 7 expands the critique into epidemiology, exposing how long-term declines in HPV-related cancers are misattributed to vaccines despite evidence that these trends predate vaccination programs and are linked to natural immunity, hygiene, and screening.
Stage 8 escalates the framework into the ethical domain, framing coercive vaccine pushing as medical genocide when severe adverse effects are ignored and data on natural immunity is deliberately suppressed.
Together, these stages reveal not only the biological impossibilities of HPV vaccine claims but also the systemic misrepresentation and ethical failures underpinning their promotion, underscoring the superiority of natural immunity and the urgent need for transparent, evidence-based public health practices.
HVBI’s Counter-Evidence
HVBI dismantles the CDC’s universality narrative by demonstrating that only about 1% of individuals are infected at any given time, and more than 95% of infections clear naturally through innate immunity. Persistence is rare, and the claim of inevitability is scientifically exaggerated. By presenting HPV as “the most common infection,” the CDC retains a distorted narrative that inflates risk perception and positions vaccines as indispensable. HVBI reframes this claim as a biological impossibility and an epidemiological misrepresentation.
Ethical Implications
Beyond biology and epidemiology, HVBI escalates the critique into the ethical domain. Stage 8 frames coercive vaccine promotion as medical genocide when severe adverse effects are ignored and natural immunity data suppressed. The CDC’s narrative of universality is not merely inaccurate; it is ethically compromised, as it justifies campaigns that undermine trust, harm populations, and ignore safer alternatives such as natural immunity and screening. By exaggerating risk and overstating vaccine efficacy, the CDC perpetuates systemic negligence and suppresses transparent public health discourse.
Conclusion
The CDC’s opening claim that HPV is “the most common sexually transmitted infection in the United States” exemplifies the Near-Universal Infection Presumption that HVBI systematically dismantles. Through its eight-stage framework, HVBI exposes the biological impossibility, epidemiological distortion, and ethical failure embedded in CDC’s messaging. Natural immunity and screening, undervalued in mainstream narratives, emerge as the true protectors.
By confronting CDC’s misinformation stage by stage, HVBI reframes the debate, revealing the superiority of natural immunity and the urgent need for transparent, evidence-based public health practices.
The Advisory Committee on Immunization Practices (ACIP), operating under the Centers for Disease Control and Prevention (CDC), has been formally renewed for a two-year period through April 1, 2028, in accordance with the Federal Advisory Committee Act of 1972. Alongside this renewal, the ACIP charter has been amended to update its operational framework, budgetary allocations, and membership provisions. Together, these actions reaffirm ACIP’s statutory authority, secure its continued existence as a federal advisory committee, and strengthen its role in shaping national immunization policy. This article analyzes both the renewal of the committee and the amendment of its charter, situating ACIP’s responsibilities within the broader context of U.S. public health governance.
Introduction
Immunization remains one of the most effective public health interventions, and the Advisory Committee on Immunization Practices (ACIP) has long been entrusted with guiding national vaccine policy. Established under the Federal Advisory Committee Act, ACIP provides expert recommendations on vaccine use, schedules, and contraindications. Its decisions carry statutory weight, shaping both federal programs and private insurance coverage. The April 2026 notice in the Federal Register is significant not only because the ACIP charter was amended but also because the committee itself was renewed for another two years, after following proper procedures and laws. This dual action underscores the enduring importance of ACIP in safeguarding public health, particularly in an era marked by rapid vaccine innovation, emerging infectious diseases, and heightened public scrutiny of immunization practices.
Governance And Membership
The amended charter specifies that ACIP may include up to nineteen members appointed by the Secretary of Health and Human Services. Members serve overlapping four-year terms, with provisions for temporary extensions to ensure continuity. Selection criteria emphasize both global geographic diversity and balance of expertise, drawing from pediatrics, internal medicine, nursing, epidemiology, biostatistics, toxicology, consumer advocacy, and public health. This diversity ensures that recommendations reflect a broad spectrum of perspectives and scientific rigor.
The charter also details the committee’s operating budget, which totals approximately $1.2 million annually. This includes federal personnel costs of $940,313, other internal costs of $140,027, member payments of $42,750, and reimbursable costs of $83,106. Such transparency in financial allocation reflects the committee’s commitment to accountability and efficient resource use.
Statutory Authority And Responsibilities
ACIP’s authority is grounded in multiple statutes. Under the Social Security Act, the committee establishes and revises the list of vaccines for children and adolescents eligible under the Vaccines for Children Program. The Public Health Service Act further mandates that ACIP recommendations adopted by the CDC Director must be covered by health insurance plans, ensuring broad access to immunizations. Additionally, Sections 311 and 317 of the Public Health Service Act authorize CDC to consult ACIP for communicable disease prevention and control. These statutory provisions highlight ACIP’s dual role as both a scientific advisory body and a policy-shaping entity.
Past Achievements And Future Directions
Between 2024 and 2025, ACIP convened six meetings and issued fifteen revised or new recommendations. These included updates to both child/adolescent and adult immunization schedules, which were subsequently published in the Morbidity and Mortality Weekly Report (MMWR) and endorsed by professional societies.
Looking ahead, the amended charter anticipates several initiatives. ACIP will convene new work groups to evaluate emerging vaccines and refine evidence-based recommendation processes. The committee will continue publishing immunization schedules and will expand opportunities for public comment, reinforcing transparency and trust. Additionally, members will receive continuing education in areas such as health economics and evidence evaluation, ensuring that recommendations remain scientifically robust and economically sound.
Analytical Discussion
The April 2026 notice is significant because it does two things simultaneously: it renews the committee itself and amends the charter under which it operates. Renewal ensures that ACIP continues to exist as a federal advisory committee with legal authority to advise on immunization practices. Without renewal, the committee would lapse, and its statutory responsibilities would be left unfulfilled. Amendment of the charter, on the other hand, updates the operational framework—clarifying membership, budget, and processes—to ensure that the committee remains effective and responsive to contemporary challenges.
This dual action highlights the importance of distinguishing between the committee as a living body of experts and the charter as its governing instrument. The committee embodies expertise, deliberation, and decision-making, while the charter provides the legal and administrative scaffolding that enables those functions. By renewing the committee and amending the charter together, the Department of Health and Human Services ensures both continuity of ACIP’s existence and modernization of its framework.
The renewal also underscores ACIP’s unique position at the intersection of science, policy, and law. Unlike many advisory bodies whose recommendations are consultative, ACIP’s guidance carries statutory authority. Once adopted by the CDC Director, its recommendations become binding for insurance coverage under the Affordable Care Act and for eligibility under the Vaccines for Children Program. This legal weight transforms ACIP from a purely scientific panel into a policy-making entity with direct consequences for access to vaccines nationwide.
The amended charter reflects a deliberate effort to maintain transparency and public trust. By publishing immunization schedules in widely accessible outlets such as the MMWR and professional society journals, ACIP ensures that its decisions are disseminated broadly to clinicians, researchers, and the public. The inclusion of opportunities for public comment further strengthens accountability, allowing stakeholders to engage with the committee’s work.
Finally, the budgetary transparency outlined in the charter reflects a broader commitment to responsible governance. By specifying personnel costs, member payments, and reimbursable expenses, the charter provides a clear picture of how resources are allocated. This openness is essential in an era when public confidence in institutions often hinges on perceptions of efficiency and accountability.
Taken together, the renewal of the committee’s tenure and the amendment of its charter reinforce ACIP’s legitimacy, adaptability, and responsiveness to contemporary challenges. The notice positions ACIP to continue serving as a trusted authority in vaccine policy, balancing scientific rigor with public accountability.
Conclusion
The April 2026 renewal of the Advisory Committee on Immunization Practices represents both continuity and evolution in U.S. immunization governance. Continuity is evident in the reaffirmation of ACIP’s statutory authority and its ongoing existence as a federal advisory committee. Evolution is reflected in the amendment of the charter, which modernizes the committee’s operational framework, enhances transparency, and expands member expertise in critical areas such as health economics.
By renewing the committee itself, the Department of Health and Human Services ensures that ACIP remains a legally constituted body capable of fulfilling its statutory responsibilities. By amending the charter, it ensures that ACIP’s processes remain current, equitable, and responsive to emerging challenges. Together, these actions secure both the institutional existence and the operational effectiveness of ACIP.
In an era of rapid biomedical innovation and persistent scientific skepticism, ACIP’s role is more vital than ever. The renewal not only secures the committee’s mandate but also strengthens its capacity to respond to future challenges. As vaccines continue to evolve and new public health threats emerge, ACIP’s balanced approach—grounded in science, informed by economics, and responsive to public concerns—will remain essential to safeguarding the nation’s health.