The Safest Vaccine In The World Is No Vaccine: TLFPGVG
Abstract
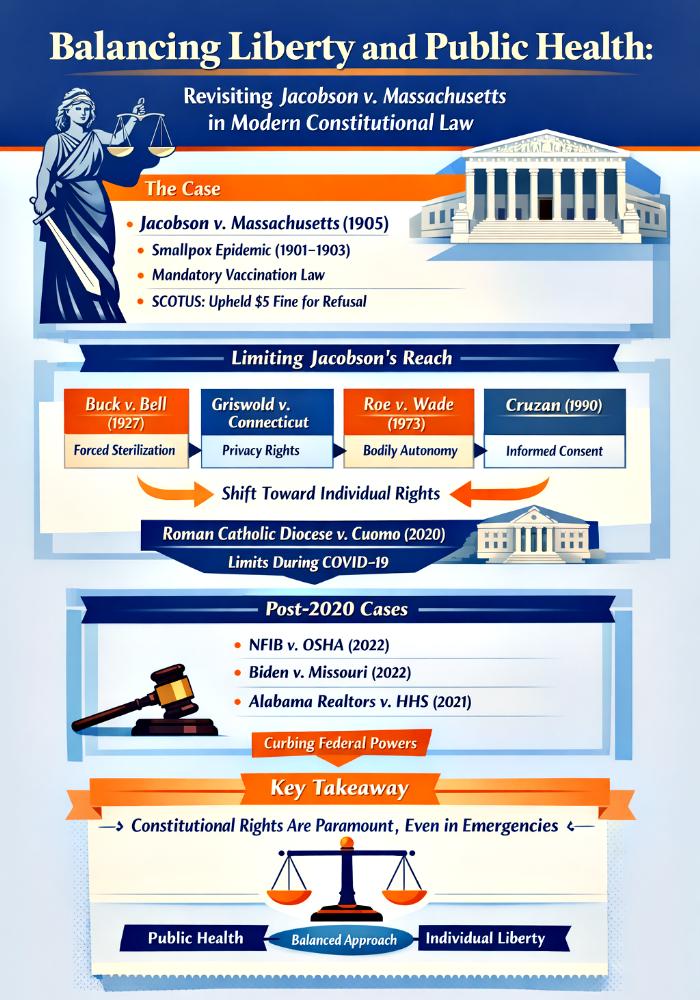
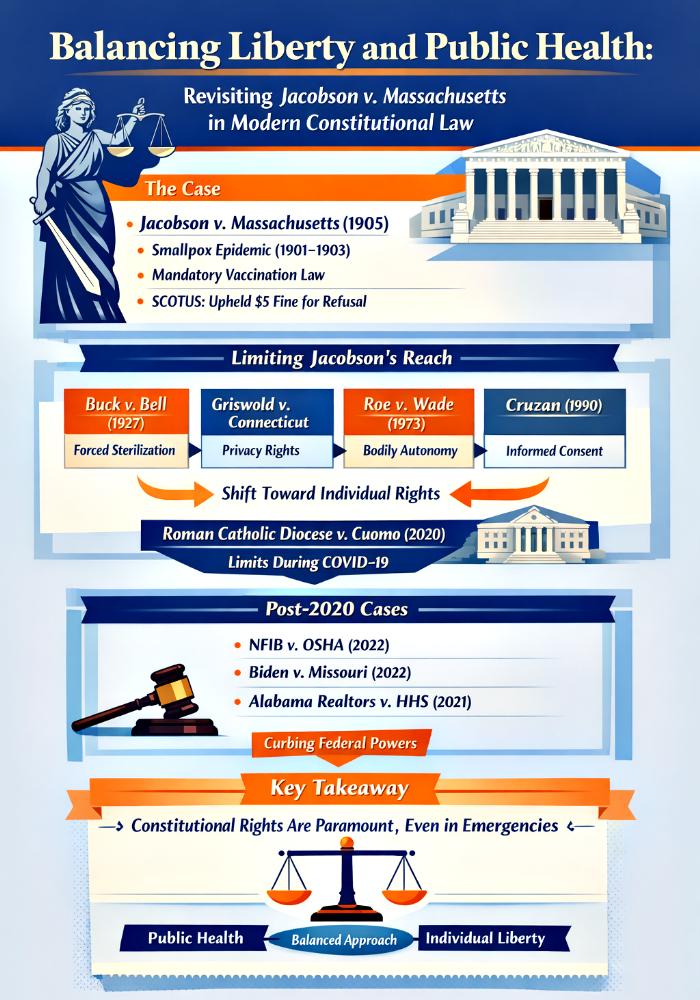
This article examines two contemporaneous Connecticut statutes—HB 5468, which establishes a regulatory framework for “equivalent instruction” (homeschooling oversight), and HB 5044, which restructures vaccine‑mandate governance by delegating nonmedical exemptions to Department of Public Health (DPH) action. Taken together, these measures illuminate a broader trend in modern statutory design: legislatures trading direct rulemaking on sensitive individual rights for administratively manageable schemes. We identify and critique what we term the “backdoor problem,” where the legislature refrains from codifying nonmedical exemptions and instead leaves them conditional on future agency rulemaking or further statutory amendment. The article situates HB 5044 and HB 5468 within historical and doctrinal contexts—Jacobson v. Massachusetts and Zucht v. King, the major‑questions doctrine, and recent Supreme Court precedents demanding statutory clarity when core liberties are implicated—and canvasses the likely constitutional claims, administrative consequences, and policy tradeoffs arising from the statutes’ design choices. Drawing on statutory text, amendment history, and constitutional doctrine, we argue that administrative precision (in the form of detailed enforcement and recordkeeping regimes) cannot substitute for legislative clarity where exemptions implicate bodily autonomy, conscience, and parental rights. This article argues that conditioning school attendance on vaccination compliance, whether in emergency or in ordinary times, is unconstitutional, violating both bodily autonomy and equal access to education. We conclude with recommendations for statutory drafting and administrative practice that restore democratic accountability and legal predictability while preserving legitimate public‑health aims.
Introduction
Over the last several legislative sessions, Connecticut has enacted measures that reveal an inclination to rely on administratively tractable frameworks when governing areas where individual autonomy and state interests collide. HB 5468 introduces a detailed system for supervising “equivalent instruction,” requiring notices, annual continuations, documentation of instruction, and routine coordination with the Department of Children and Families (DCF). HB 5044, by contrast, articulates a robust medical‑exemption process while expressly leaving nonmedical exemptions (religious and philosophical) either to future statutory amendment or to DPH rulemaking.
The juxtaposition is striking: one statute enlarges the state’s capacity for oversight of parenting and education choices; the other centralizes the power to define exemptions from medical compulsion within an administrative agency rather than the legislature itself. Both choices reveal a preference for administrative convenience and procedural uniformity over the kind of legislative clarity and entrenchment that protect fundamental liberties.
The stakes of this design choice are high. Exemptions from state coercion—especially medical mandates—bear directly on bodily autonomy, freedom of conscience, and parental authority. When legislatures leave the existence, scope, or procedural safeguards for those exemptions to forthcoming agency rules, they convert prospective rights into contingent permissions. This article argues that such delegation produces a “backdoor problem”: rights that should be statutory entitlements become effectively controlled by administrative fiat, undermining predictability, democratic accountability, and constitutional protection.
Constitutional Violations By The Proposed Connecticut Statutes
(1) Statutory Architecture: HB 5468 And HB 5044
HB 5468 constructs a supervisory architecture over homeschooling by requiring parents to file notices, submit annual affirmations, maintain instructional documentation, and route school withdrawals into DCF awareness. HB 5044 adopts a dual‑track approach to vaccine exemptions: codifying medical exemptions with clear safeguards while leaving nonmedical exemptions conditional on later statutory change or DPH rulemaking.
(2) The Backdoor Problem: Doctrine And Democratic Accountability
Delegation is a common feature of modern governance, but constitutional problems arise when delegation affects decisive issues tied to fundamental rights. Exemptions from compulsory medical interventions implicate bodily integrity and religious liberty—domains where courts demand statutory clarity. HB 5044 risks treating exemptions as discretionary regulatory concessions rather than legislatively guaranteed rights, thereby weakening democratic accountability.
(3) Interplay And Mutual Reinforcement
Taken together, HB 5468 and HB 5044 reveal a coordinated administrative thrust: routinized state contact with families choosing alternative education paths and concentrated agency power over exemptions. The common effect is expanded oversight of private family choices, increased data collection, and narrower zones of statutory protection.
(4) Litigation And Administrative Implementation
Challenges to HB 5044 will likely focus on excessive delegation, invoking separation‑of‑powers grounds and the major‑questions doctrine. Claims against HB 5468 will center on parental rights, due process, and privacy concerns. Administrative‑law claims could include challenges to rulemaking that narrows exemptions to the point of elimination.
Relevant Tables: Mapping Power And Rights In Connecticut’s Administrative Turn
Before presenting the comparative tables, it is important to situate them as analytical tools. The tables below synthesize how HB 5468 and HB 5044 allocate authority, affect rights, and produce enforcement consequences. They are not mere descriptive charts but frameworks for understanding how statutory design choices translate into lived realities for families, agencies, and courts. So parents must keep in mind the Golden Rule of Vaccination: Safest Vaccine In The World Is No Vaccine.
Table 1: Where Power Lands—Allocation, Procedure, And Rights
| Dimension | HB 5468 (Equivalent Instruction) | HB 5044 (Vaccine Mandate Framework) |
|---|---|---|
| Primary decision‑maker | Legislature sets framework; districts/DOE/DCF implement | Legislature sets medical exemptions; DPH defines nonmedical exemptions |
| Key procedural mechanisms | Notices, annual continuation, documentation, district review, DCF checks | Codified medical exemptions; delegation to DPH for nonmedical exemptions |
| Rights implicated | Parental rights, privacy, educational choice | Bodily autonomy, religious conscience |
| Predictability | Moderate: clear procedures but discretionary implementation | Low: medical exemptions predictable; nonmedical exemptions contingent |
| Legal risks | FERPA/privacy, due process, parental rights | Delegation challenges, equal protection, religious liberty |
Analysis:
Table 1 highlights the asymmetry in legislative specification. HB 5468 is administratively dense, prescribing notices, documentation, and district/DCF roles, thereby creating many procedural touchpoints that are predictable in form but variable in application. This produces clearer short‑term expectations but also expands the number of discretionary actors whose interpretations will determine outcomes, making uniform protection of parental rights dependent on implementation fidelity.
By contrast, HB 5044 concentrates a consequential choice—the existence and scope of nonmedical exemptions—within DPH’s rulemaking authority. The table underscores the resulting predictability gap: medical exemptions are statutorily secure, whereas nonmedical exemptions are conditional and legally unstable. That instability shifts the balance of power toward administrative decisionmakers and away from legislative accountability at precisely the moments when constitutional liberties are most implicated.
Table 2: Litigation Vectors, Administrative Actions, And Family Impacts
| Litigation Vector | Likely Administrative Response | Practical Impact on Families |
|---|---|---|
| Delegation challenge to HB 5044 | DPH may delay or narrow rules | Acute uncertainty about exemptions |
| Parental‑rights claims against HB 5468 | Districts/DOE issue protocols | Increased administrative encounters |
| FERPA/privacy disputes | Agencies negotiate compliance | Concerns about record sharing |
| Religious‑liberty suits | DPH crafts narrow exemption rules | Risk of exclusion from school/work |
| Administrative‑law challenges | Agencies produce extensive records | Policy volatility during rulemaking |
Analysis:
Table 2 maps how litigation and administrative behavior are likely to unfold. HB 5044 invites major‑questions and delegation challenges aimed squarely at the statute’s conditional approach to nonmedical exemptions. The administrative response could be to issue either deliberately narrow rules to restrict exemptions or broader rules to preserve them, but either path will encounter legal scrutiny and produce practical uncertainty for affected individuals in the interim.
For HB 5468, the table shows a multiplicity of legal fronts—privacy, parental rights, procedural due process—arising from routine data sharing and DCF screening. Administratively, districts and DCF will need to develop protocols that comply with federal privacy law while meeting statutory reporting obligations. Resource constraints and local discretion almost certainly produce uneven implementation, adding to families’ compliance burdens and amplifying the risk of contested removals or investigations.
Conclusion
HB 5468 and HB 5044 together exemplify a legislative technique that privileges administrative precision while deferring quintessentially normative decisions—those involving exemptions that touch bodily autonomy, religious conscience, and parental authority—to agencies. This is the “backdoor problem”: when crucial rights are not codified comprehensively by legislatures, they become subject to regulatory discretion and therefore vulnerable to erosion without the safeguard of explicit statutory protections and democratic accountability.
The likely consequences are predictable: increased administrative intrusion into private family life, uneven local implementation, significant litigation challenging delegated authority, and legal uncertainty for affected individuals. For lawmakers and administrators concerned with both public health and constitutional fidelity, the solution is straightforward in principle though politically difficult in practice: legislate the contours of nonmedical exemptions clearly, limit routine data sharing to cases with articulable child‑safety concerns, and reserve for the legislature the power to resolve politically salient tradeoffs that implicate fundamental rights.
Administrative agencies should be tasked with implementing—but not deciding—the existence of rights. Doing so restores predictability, preserves democratic accountability, and ensures that decisions about who may be compelled by the state to accept medical interventions remain subject to the deliberative processes our constitutional structure contemplates. Without that corrective, HB 5044 risks converting exemptions from statutory entitlements to contingent administrative favors, and HB 5468 exemplifies how oversight regimes can compound that shift—together charting a course toward administrative control where legislative clarity and constitutional protection are most needed.